Ciencias Psicológicas; v20(1)
January - June 2026
10.22235/cp.v20i1.4723
Original Articles
MotoTiles: A Tool for Cognitive and Motor Stimulation in Active Aging
MotoTiles: una herramienta de estimulación cognitiva y motora en el envejecimiento activo
Mototiles: uma ferramenta de estimulação cognitiva e motora no envelhecimento ativo
Ana María Salazar1, ORCID 0000-0003-1288-1469
Fidel Mauricio Bonilla2, ORCID 0000-0003-4324-3224
Daniel Felipe Carvajal Tavera3, ORCID 0009-0001-0872-6362
Milagros Castillo4, ORCID 0009-0007-4713-4566
Camila Grosso5, ORCID 0009-0006-4319-3684
Janeth Jiménez6, ORCID 0009-0005-0676-4129
Angela Patricia Romero7, ORCID 0009-0009-8149-5431
Jhoanna Lizeth Vargas8, ORCID 0009-0000-5754-2669
1 Universidad El Bosque, Colombia, [email protected]
2 Universidad El Bosque, Colombia
3 Universidad El Bosque, Colombia
4 Universidad El Bosque, Colombia
5 Universidad El Bosque, Colombia
6 Universidad El Bosque, Colombia
7 Universidad El Bosque, Colombia
8 Universidad El Bosque, Colombia
Abstract:
Technology-based cognitive training has emerged as an innovative strategy to enhance mental capacities across various populations. In this context, the Technical University of Denmark developed MotoTiles, an interactive tool aimed at strengthening cognitive and motor functions through playful activities, whose utility has been documented for preventing cognitive decline among older adults. Based on this technology, a prospective experimental study was conducted using a randomized 2 × 2 mixed factorial design, with pre- and post-intervention assessments in both an experimental group and a waitlist control group. The sample consisted of 51 participants with a mean age of 68 years. The results suggest that cognitive training using MotoTiles may contribute to improvements in cognitive and motor functions in adults over the age of 50, particularly in alternating and divided attention, cognitive processing speed, and gait velocity. Although some variables did not reach statistical significance, favorable trends were observed that support the potential of this type of intervention. It is concluded that MotoTiles represents a promising tool within the framework of active aging, and future research is recommended to increase sample size and training intensity to optimize its impact and strengthen empirical evidence of its effectiveness in this population.
Keywords: older adults; cognitive training; motor training; attention; visuospatial skills; cognitive stimulation.
Resumen:
El entrenamiento cognitivo basado en tecnología se ha consolidado como una estrategia innovadora para optimizar las capacidades mentales en diversas poblaciones. En este contexto, la Universidad Técnica de Dinamarca desarrolló MotoTiles, una herramienta interactiva orientada al fortalecimiento de funciones cognitivas y motoras mediante el juego, cuya utilidad ha sido documentada en la prevención del deterioro cognitivo en personas mayores. Con base en esta tecnología, se llevó a cabo un estudio experimental prospectivo con un diseño factorial 2 × 2 mixto aleatorizado, con mediciones pre y post intervención tanto en un grupo tratamiento como en un grupo control en lista de espera. La muestra estuvo conformada por 51 participantes con una edad media de 68 años. Los resultados sugieren que el entrenamiento cognitivo mediante el uso de MotoTiles puede favorecer la mejora de funciones cognitivas y motoras en adultos mayores de 50 años, en particular en procesos como la atención alternante y dividida, la velocidad de procesamiento cognitivo y la velocidad de la marcha. Aunque algunas variables no alcanzaron significancia estadística, se observaron tendencias favorables que respaldan la utilidad de este tipo de intervenciones. Se concluye que MotoTiles representa una herramienta prometedora en el contexto del envejecimiento activo, y se recomienda que futuras investigaciones amplíen el tamaño muestral y la intensidad del entrenamiento, a fin de optimizar su impacto y fortalecer la evidencia empírica sobre su efectividad en esta población. Palabras clave: ancianos; entrenamiento cognitivo; entrenamiento motor; atención; habilidades visoespaciales; estimulación cognitiva.
Resumo:
O treinamento cognitivo baseado em tecnologia consolidou-se como uma estratégia inovadora para otimizar as capacidades mentais em diversas populações. Nesse contexto, a Universidade Técnica da Dinamarca desenvolveu o MotoTiles, uma ferramenta interativa voltada ao fortalecimento de funções cognitivas e motoras por meio do jogo, cuja utilidade tem sido documentada na prevenção do declínio cognitivo em idosos. Com base nessa tecnologia, realizou-se um estudo experimental prospectivo com delineamento fatorial misto randomizado 2 × 2, com medições pré e pós-intervenção tanto em um grupo de tratamento quanto em um grupo controle em lista de espera. A amostra foi composta por 51 participantes com idade média de 68 anos. Os resultados sugerem que o treinamento cognitivo por meio do uso do MotoTiles pode contribuir para melhorias nas funções cognitivas e motoras em adultos com mais de 50 anos, em particular em processos como atenção alternada e dividida, velocidade de processamento cognitivo e velocidade da marcha. Embora algumas variáveis não tenham alcançado significância estatística, observaram-se tendências favoráveis que respaldam a utilidade desse tipo de intervenção. Conclui-se que o MotoTiles representa uma ferramenta promissora no contexto do envelhecimento ativo, e recomenda-se que futuras pesquisas ampliem o tamanho da amostra e a intensidade do treinamento, a fim de otimizar seu impacto e fortalecer a evidência empírica sobre sua eficácia nessa população.
Palavras-chave: idosos; treinamento cognitivo; treinamento motor; atenção; habilidades visoespaciais; estimulação cognitiva.
Received: 04/07/2025
Accepted: 04/02/2026
Cognitive abilities are not static, and age is a key factor in their decline. From the age of 50 onward, a progressive deterioration in various cognitive functions can be observed—a phenomenon known as age-related cognitive decline (Knopman et al., 2009; National Institute on Aging, 2023; NeuronUp, 2024). This decline is associated with morphological, metabolic, and physiological changes in the brain, influenced by both hereditary factors and individual experiences, as well as contextual, psychological, and emotional aspects (Barlow, 2000; Peters, 2009).
The progression of this decline constitutes a risk factor for the development of neurodegenerative diseases such as dementia, which significantly impact functionality and quality of life in affected individuals (Feldberg et al., 2020). Therefore, it is essential to develop preventive and intervention strategies. One of the most effective techniques in this field is cognitive training, defined as a set of activities designed to preserve or improve individuals' cognitive abilities (Feldberg et al., 2020). The implementation of cognitive training programs in older adults has shown positive effects on their functionality and autonomy, promoting a better quality of life (Cruz-Peralta & González-Celis, 2023). In this line of research, technology-based cognitive training has emerged as an innovative tool to enhance mental capacities across various populations.
In this context, Dr. Henrik Hautop Lund of the Technical University of Denmark developed MotoTiles (Moto), an interactive tool aimed at training cognitive and motor functions through a variety of games. This system consists of ten interactive tiles that can communicate with each other, be configured in different combinations, or be used independently, allowing users to develop strategies to improve their performance and stimulate their cognitive abilities (Entertainment Robotics, 2014).
The use of MotoTiles has been documented in different parts of the world and across populations with various physical and cognitive conditions, yielding favorable results (Jessen & Lund, 2017; Liu et al., 2018; Lund et al., 2020a; Lund et al., 2020b; Lund & Jessen, 2014; Wang et al., 2021). Studies such as that by Piech and Czernicki (2021) indicate that MotoTiles enhance cognition in older adults. Lund (2015) also demonstrated its usefulness in older adults with mild dementia. These findings suggest that interaction with the tool enhances participation and intrinsic motivation, promoting sensory and cognitive stimulation. Additionally, it improves physical condition by strengthening muscles, optimizing balance, and fostering motor functionality, thereby contributing to fall prevention (Ehrari et al., 2020; Jessen & Lund, 2017).
Some intervention protocols using this tool suggest that engaging in playful exercises with MotoTiles for 12 minutes, twice a week for 10 weeks, can improve cognitive and motor performance in older adults (Ehrari et al., 2020). On the other hand, Liu et al. (2018) found that frequent use of MotoTiles led to significant improvements in tasks related to attention and visual processing, although improvements in memory were inconclusive due to difficulties participants had in understanding the games.
Moreover, recent studies highlight the relevance of processing speed as a key component of cognitive performance, as it directly influences the efficiency of various executive functions (Silva-Fernandes et al., 2022). In this regard, stimulation strategies such as those offered by MotoTiles may play a crucial role in optimizing cognition in the older adult population.
Therefore, the aim of this study was to evaluate the impact of a cognitive and motor training program using the MotoTiles tool on cognitive performance and motor functionality in individuals over the age of 50.
Materials and Methods
A prospective experimental study was conducted using a randomized 2 × 2 mixed factorial design (Hernández-Sampieri & Mendoza, 2018). Two measurements were taken: an initial pre-intervention assessment (M1), and a second assessment conducted two months after completion of the MotoTiles training (M2).
The sample consisted of 52 individuals over the age of 50, with a mean age of 68.7 years and an average of 15.17 years of education. Thirty-nine participants (75 %) were women residing in the city of Bogotá. Participants were randomly assigned to one of two groups: the treatment group (TG), composed of 26 individuals, calculated based on a large effect size of 0.8 and an alpha of .05 according to Cohen's criteria (1992), who received the MotoTiles intervention; and the waitlist control group (CG), consisting of 26 individuals with characteristics similar to those of the TG.
Inclusion and exclusion criteria
Literate older adults capable of understanding and following instructions were included. Individuals were excluded if they were illiterate, displaced, or institutionalized, as well as those with uncorrected auditory and/or visual impairments. Also excluded were participants with vertigo, nausea, dizziness, balance issues, or disabling motor difficulties requiring assistive devices (e.g., crutches, canes, or wheelchairs). Additionally, individuals with moderate or severe cognitive impairment—verified through the administration of the Mini-Mental State Examination (MMSE; Escobar et al., 1999)—were excluded.
Procedure
This study was approved by the Ethics Committee of Universidad El Bosque under code PCI 2023-0026. All ethical requirements for research involving human subjects established by Colombian legislation were met, in accordance with the guidelines of the Declaration of Helsinki and Resolution 8430 of 1993 on human subjects research (Ministerio de Salud, 1993), with a minimal risk classification.
Participants over 50 years of age enrolled in the active aging program of the Compensar family compensation fund in Bogotá, Colombia, were invited to participate via word of mouth. Those who voluntarily agreed to participate, after signing informed consent, were scheduled for individual appointments at Compensar facilities, where they were assessed by final-semester psychology students under the supervision of licensed psychologists who were previously trained in the administration and interpretation of the evaluation protocol.
Each participant was assigned a numeric code to protect their identity. Group randomization was conducted using the free online platform Sealed Envelope. The intervention then began, with its structure detailed in Table 1. Based on the intervention protocols described by Lund et al. (2020a), which recommend between 8 and 12 sessions, this study implemented 10 MotoTiles training sessions for the treatment group. Each session was led by at least one psychologist from the research team, conducted once per week, and lasted 60 minutes.
The following outlines the phase-specific structure of the intervention to ensure methodological replicability:
1. Warm-up and Cool-down Phase: Duration 10 minutes, each session began and concluded with a standardized stretching and cool-down routine (5 minutes at the beginning and 5 minutes at the end).
2. Central Training Phase: Duration 50 minutes, this phase involved the specific rotation of two to three games per session. Games were administered in individual or pair formats, with difficulty levels dynamically adjusted to ensure adaptive training progression. Each game targeted specific objectives of dual-task training (cognitive and motor), including the stimulation of sustained attention, working memory, and cognitive-motor processing speed.
3. Home Reinforcement Phase: Upon completion of each session, participants were provided with a written protocol detailing ecological and practical activities. These tasks were designed to reinforce the specific cognitive or motor skills addressed during the session, promoting their integration into daily life activities.
A detailed description of the games, the cognitive functions stimulated, and the motor domains are presented in Table 1, and the overall procedure is schematically illustrated in Figure 1.
Control Group Intervention Protocol: The control group was subjected to a low-intensity cognitive training protocol, which was designed to control the effects of attention and social interaction. The protocol consisted of a total of four standardized sessions, administered once per week. The intervention was conducted using the computerized platform CogniFit, a commercially available program focused on training specific cognitive functions (such as attention, working memory, and processing speed). During each session, participants individually performed the exercises proposed by the platform, remaining seated in front of a computer for a period of 45 minutes.
Figure 1: Flow diagram of the study procedure phases
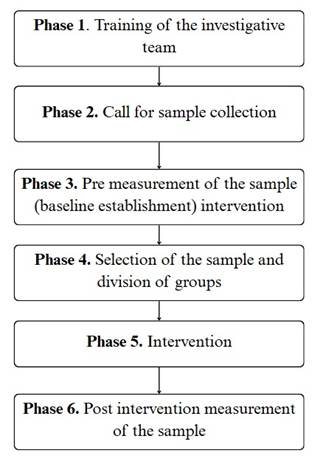
Table 1: Games Used in the Cognitive Training Sessions with MotoTiles
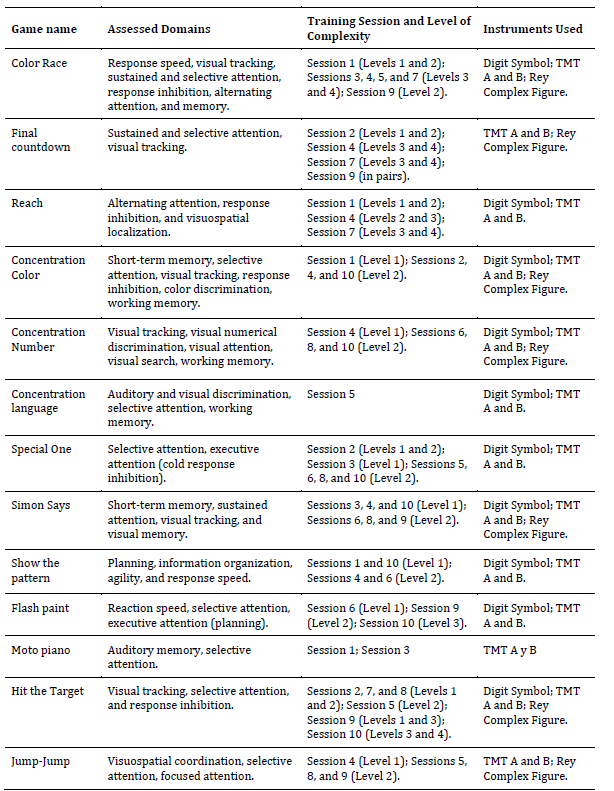
Note: Information taken from the Moto Tiles Manual (Entertainment Robotics, 2014); for videos and more details, visit <https://www.Moto-tiles.com/>.
On the other hand, the waitlist control group was offered a simple and low-intensity training program (four sessions) based on the use of the computerized program CogniFit; participation was voluntary. Similarly, after the post-intervention assessment was completed for both groups, participants in the control group were offered additional training sessions using the Moto protocol, with voluntary participation.
Instruments
Demographic and Inclusion Criteria Questionnaire. This questionnaire was designed by the research team for the purpose of collecting general information such as gender, age, and educational level. It also included questions related to potential cognitive and/or motor conditions that could hinder participation in the study.
Cognitive Change Complaint Questionnaire (QCC). The QCC, developed and validated by Salazar and Maldonado (2020), assesses the subjective perception of cognitive changes across three dimensions: (1) cognitive, (2) global functioning, and (3) emotional. It consists of 26 items and has a cutoff score of 51. Its reliability was determined using Cronbach’s alpha coefficient, yielding high internal consistency (α = .973), along with 96.8 % sensitivity and 96.1 % specificity.
Rey Complex Figure (copy and recall). This test was developed by André Rey in 1941 and later standardized by Osterrieth in 1944. It evaluates visual perception and memory using 18 elements scored for correct location and accuracy (Osterrieth, 1944). The test was validated in Colombia by Arango-Lasprilla et al. (2022), showing a reliability coefficient of 0.85 for the copy phase and .97 for the recall phase.
Montreal Cognitive Assessment (MoCA). The MoCA is a brief screening tool that is both sensitive and specific for detecting mild cognitive impairment and dementia in older adults. Developed by Nasreddine et al. in 2005, it assesses memory, attention, language, visuospatial ability, task execution, and abstract thinking. It consists of 30 items. Although the general cutoff score is < 26, for this study a threshold of < 24 was adopted based on the Colombian validation by Pedraza et al. (2016), which reported moderate test-retest reliability (.62) and good internal consistency (.85).
Ineco Frontal Screening (IFS). The IFS is a neuropsychological battery developed by the Institute of Cognitive Neurology (Torralva et al., 2009) to assess executive functions. It comprises eight subtests with a maximum score of 30 points. The Colombian validation by Zapata-Zabala et al. (2019) was used in this study, which establishes a cutoff of < 23 to identify frontal dysfunction. The test demonstrated strong discriminatory power under the ROC curve (AUC = 0.93, p < .001), with 80 % sensitivity and 91 % specificity.
Symbol Digit Modalities Test (SDMT). Developed by Smith in 1973 and validated in Colombia by Arango-Lasprilla et al. (2015), the SDMT assesses sustained attention, visual scanning, and perceptual speed. The test presents nine geometric figures, each paired with a number, and participants are required to correctly match them as quickly as possible. Although originally administered in 90 seconds, the time was extended to 120 seconds in this study, following the Colombian validation by Arango-Lasprilla et al. (2022). Among older adults, reliability ranges from .263 to .351. The test shows good convergent validity with the WISC-R and Stroop tests, and a test-retest correlation of approximately .80 in healthy populations.
Trail Making Test (TMT). Created by Reitan and Wolfson (1985) and validated in Colombia by Arango-Lasprilla et al. (2015), the TMT assesses visual attention, processing speed, cognitive flexibility, and executive functions. It is divided into two parts: TMT-A (sustained attention) and TMT-B (alternating attention with executive demands). The test demonstrates high reliability: r = .99 for TMT-A and r = .93 for TMT-B. Construct validity was confirmed via factor analysis in the Colombian validation by Arango-Lasprilla et al. (2022).
Instrumented Timed Up and Go (iTUG). Functional mobility and balance were assessed using the iTUG test, which employed inertial measurement units (IMUs) from the Xsens brand. These sensors, placed on eight body regions, recorded acceleration, rotation, and magnetic field data. For kinematic analysis, only the data from the sensor positioned on the pelvis were used due to its proximity to the center of mass and the quality of recorded signals.
Statistical analysis
Cognitive data were analyzed using Jamovi software (version 2023). Prior to inferential analysis, the normality of distributions was tested using the Shapiro-Wilk test, appropriate for samples with over 50 participants. Results indicated that cognitive variables followed a non-parametric distribution.
Descriptive statistics (mean, standard deviation, frequencies, and percentages, as appropriate) were used to describe the sample's demographic characteristics. To explore relationships between key variables and control for potential sources of variability, linear mixed models were applied, using sociodemographic variables as covariates. The models included mean scores for each test, along with significance levels associated with treatment effects, time of measurement, and interaction. This approach enabled the incorporation of both fixed effects (related to the study’s main independent variables) and random effects (associated with inter- and intra-individual variability), providing a robust and flexible statistical framework for the analysis of longitudinal and/or clustered data.
The use of linear mixed models allowed for the precise evaluation of intra- and inter-group differences, effectively controlling sample heterogeneity and optimizing the interpretation of results in line with the study objectives. All analyses were conducted using a statistical significance level of p < .05.
Motor data were processed using specialized motion analysis software. Variables such as total test time and gait characteristics (e.g., velocity, cadence, number of steps) were assessed, with outbound and return phases analyzed separately in order to build a detailed profile of gait patterns. Linear mixed models (LMMs) were also used to compare pre- and post-intervention measurements, accounting for repeated measures and individual variability (UCLA, 2025). To control Type I error in multiple comparisons, the Holm-Bonferroni correction was applied. Compared to the traditional Bonferroni method, this approach is less conservative and better preserves statistical power in small samples (Editverse, 2025).
Cognitive results
Table 2 presents the average scores obtained on the cognitive tests before and after the intervention for both groups. A slight improvement was observed in the post-intervention scores of the treatment group, particularly in the MoCA, INECO, and the memory component of the Rey Complex Figure test. In addition, a reduction in subjective cognitive complaints was noted, as measured by the Cognitive Change Complaint Questionnaire (QCC).
Table 2: Average Cognitive Scores in Pre- and Post-Intervention Assessments for Both Groups
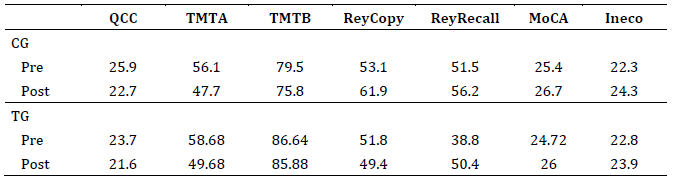
Note: CG: waitlist control group; TG=treatment group; QCC: Cognitive Change Complaint Questionnaire; TMTA and TMTB: Trail Making Test A and B; ReyCopy: Rey Complex Figure (copy); ReyRecall: Rey Complex Figure (recall); MoCA: Montreal Cognitive Assessment Test.
The significance analysis (Table 3) showed that the intervention group obtained an estimated change score of -0.9166 on the MoCA test, suggesting a slight improvement in the post-test compared to the pre-test. However, the 95 % confidence interval (-3.5651 to 1.7320) included the null value, indicating that the difference did not reach statistical significance. Among the covariates analyzed, educational level showed a significant association with cognitive performance, suggesting that a higher level of education is related to better results on cognitive tests.
In the Trail Making Test A (TMT-A), statistical significance was not reached (p = .095), although a trend was observed that may be relevant in studies with a larger sample size. For the Trail Making Test B (TMT-B), education again showed a significant association (p = .035). In the Symbol Digit Modalities Test (SDMT), both age (p < .001) and education (p < .001) were significantly associated with better performance, highlighting the influence of these factors on alternating attention and processing speed.
Table 3: Correlation Between Study Variables and the MoCA, TMT A and B, and SDMT Tests
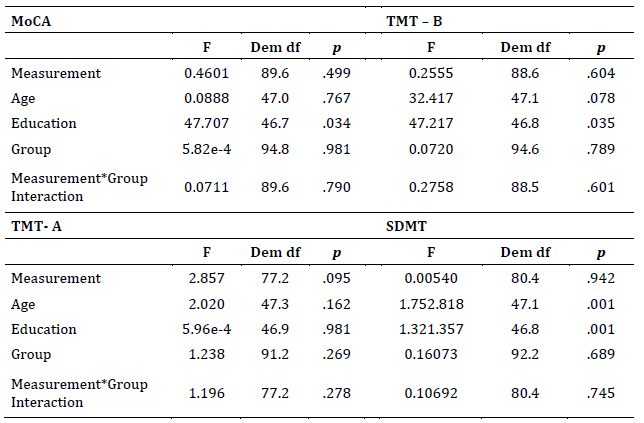
Note: MoCA: Montreal Cognitive Assessment Test; TMA A and B: Trail Making Test A and B; SDMT: Symbol Digit Modalities Test. *p <= .05
Regarding the Rey Complex Figure (Table 4), the results indicated that both age (p = .017) and education (p < .001) were significantly associated with performance in the delayed recall phase. In the copy phase, only education showed a significant relationship (p = .012). These findings reinforce the importance of educational level and age in visuospatial and memory task performance.
Table 4: Correlation Between Study Variables and the Rey Complex Figure Test (Copy and Delayed Recall)
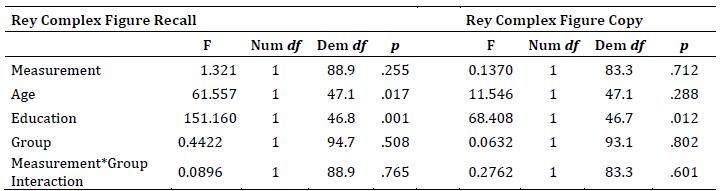
*p <= .05
Taken together, the cognitive results suggest that the intervention led to slight improvements in the experimental group, although most tests did not reach statistical significance. Education emerged as a key factor associated with better cognitive performance, while age primarily influenced tasks involving memory and processing speed. These observations are consistent with previous literature highlighting the moderating role of sociodemographic variables in cognitive performance.
Motor results
Table 5 summarizes the results of the pre- and post-intervention motor assessments for both groups, analyzed in a subsample of 28 participants (7 in the control group and 21 in the experimental group). In the experimental group, statistically significant differences were identified in two key indicators: gait speed (p = .030) and total walking time (p = .027).
These changes suggest a modification in participants' motor strategy following the intervention, possibly aimed at optimizing stability or adapting to neuromuscular demands. Although variables such as step length, number of strides, and stride length did not reach statistical significance, a trend toward a more conservative gait pattern was observed in the experimental group.
In contrast, the control group did not show significant differences between pre- and post-intervention measurements, which supports the hypothesis that the changes observed in the experimental group are attributable to the intervention.
Table 5: Pre- and Post-Intervention Comparison of Motor Outcome Variables
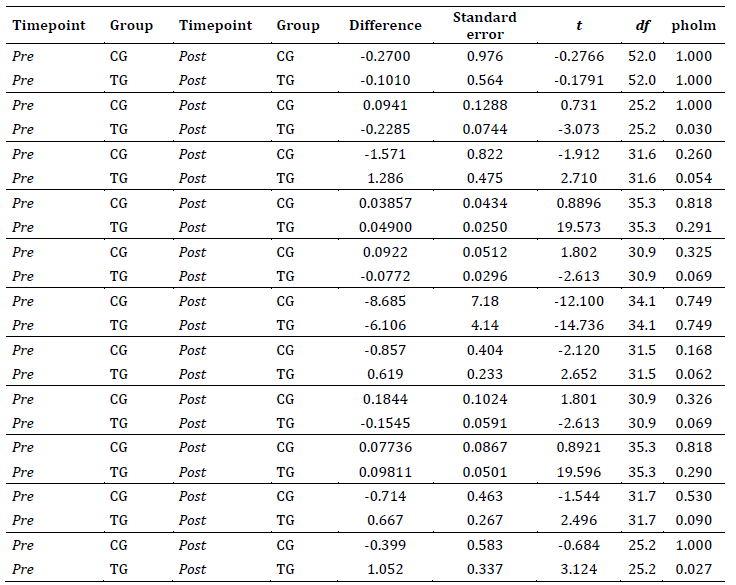
Note: TG: treatment group; CG: waitlist control group.
The motor results indicate that the intervention had a positive and significant impact on gait speed and walking time in the experimental group. These changes may reflect a favorable adaptation in motor strategy aimed at maintaining stability and safety during gait key aspects in populations vulnerable to motor impairments.
Discussion
The present study evaluated the impact of a cognitive and motor training program using the MotoTiles tool in older adults, analyzing both cognitive and motor performance after ten intervention sessions. The results showed a slight improvement in cognitive scores and significant changes in motor parameters, suggesting the potential utility of multimodal interventions in this population.
Cognitive performance
In the cognitive domain, a slight improvement was observed in MoCA scores, as well as in the INECO test and the memory item of the Rey Complex Figure, alongside a reduction in subjective cognitive complaints. Although the difference in MoCA was not statistically significant, other tests such as TMT-A showed only a trend toward statistical significance (p = .095), which could be attributed to the limited sample size and insufficient statistical power to detect subtle changes. In terms of cognitive functions, the improvements observed in these tests are attributed to a positive impact on general cognition, sustained attention, visuoconstructional processes, and reduced reaction time.
These findings are consistent with previous studies reporting modest positive effects of cognitive interventions in older adults, particularly when training frequency and duration are moderate (Liu et al., 2018). These results also align with previous MotoTiles studies reporting selective improvements in attention, visuospatial processing, and reaction speed (Liu et al., 2018), particularly when interventions are implemented with similar session frequency and duration. Furthermore, education and age were found to significantly influence cognitive performance, reinforcing the concept of cognitive reserve and the importance of sociodemographic factors in the response to cognitive interventions (Johnson et al., 2019; Smith et al., 2020). This pattern aligns with literature on age-related cognitive trajectories. Salthouse (2019) highlights that processing speed, attentional capacity, and memory typically decline with advancing age. In this context, even modest gains, as observed in the present study, may be clinically meaningful, as they counteract the expected downward trend associated with normal aging. Moreover, in aging populations, the mere maintenance of baseline cognitive performance is considered a positive outcome, as it indicates resilience against the progressive decline typically observed over time. This perspective reinforces the relevance of the present findings, even when improvements are modest or non-significant from a statistical standpoint.
Similarly, Arokiaraj et al. (2020) reported that computerized cognitive training in healthy older adults tends to produce small-to-moderate improvements, particularly in processing speed and attentional domains, when training intensity and duration are comparable to those used in the present study. Likewise, meta-analytic findings by Chan et al. (2024) indicate that technology-based cognitive training yields modest yet meaningful effects on memory and other cognitive functions in older adults with cognitive impairment, further supporting the pattern of selective gains observed here. Comparable patterns have also been observed in studies where gains in memory or executive functioning did not reach statistical significance, often due to the cognitive complexity of the tasks involved or the limited familiarity participants had with game-based activities (Liu et al., 2018).
Motor performance
Regarding motor outcomes, statistically significant differences were identified in gait speed (p = .030) and total walking time (p = .027) in the experimental group, while other variables such as step length and number of strides showed non-significant trends. These findings suggest that participants modified their motor strategies, possibly adopting a more conservative gait pattern as a compensatory mechanism to maintain stability or respond to new neuromuscular demands following the intervention. The literature supports that both physical and cognitive interventions can induce functional adaptations in gait patterns, especially in older adults with biomechanical or neuromotor alterations (Eggenberger et al., 2015). In particular, Eggenberger et al. (2015) demonstrated that simultaneous cognitive–motor training can enhance gait velocity and stability, a result that closely mirrors the improvements seen in the present study and further reinforces the value of dual-task–oriented approaches like MotoTiles. Thus, previous MotoTiles interventions have shown improvements in balance, coordination, and fall-prevention–related motor parameters (Ehrari et al., 2020; Lund et al., 2020a), which supports the functional relevance of the gait changes observed here. The absence of significant changes in the control group further supports the hypothesis that the observed modifications are directly related to the intervention.
Finally, the clinical and social relevance of this study and its findings should be highlighted. Cognitive and motor training using MotoTiles represents an innovative and accessible strategy to promote overall health in older adults, contributing to both the prevention and slowing of cognitive and motor decline associated with aging. Clinically, the findings suggest that this type of intervention may help preserve executive functions, attentional processes, and processing speed (as reflected in reaction times), as well as improve key motor parameters such as gait speed factors that translate into greater autonomy and reduced risk of dependency and falls. Socially, the implementation of interactive and group-based programs like MotoTiles fosters active participation, a sense of belonging, and social integration crucial elements for combating isolation and improving quality of life in old age. Moreover, the adaptability of the intervention to different educational levels and functional capacities broadens its applicability and potential public health impact, helping to reduce the socioeconomic burden associated with disability and functional decline in aging populations.
Conclusions
In summary, cognitive and motor training using MotoTiles demonstrated a positive impact on cognitive function and selected motor parameters in adults over the age of 50, emphasizing the relevance of alternating attention, processing speed, and gait as intervention-sensitive indicators. Education and age were confirmed as key moderating factors of performance. Likewise, the study provides relevant evidence for the design of preventive and therapeutic strategies in geriatric care, promoting the integral health and social integration of older adults. The implementation of cognitive and motor stimulation programs, especially those that incorporate playful and technological components, represents a promising and well-received intervention approach for this population. These conclusions are consistent with prior evidence showing that combined cognitive–motor approaches can produce benefits even with moderate training intensities, reinforcing the value of multimodal interventions in aging populations. They also highlight the feasibility of introducing technology-based cognitive–motor training in community and clinical settings, offering an accessible and engaging option for programs seeking to promote functional aging.
Future studies with larger samples, increased session frequency, more sensitive measurement tools, and longitudinal follow-up will allow for validation and further exploration of these findings, ultimately optimizing the design of training programs aimed at older adult populations. Future work should also explore whether more intensive or dual-task–focused protocols using MotoTiles or similar technologies can generate stronger or longer-lasting effects across cognitive and motor domains.
Limitations
The current study identified several methodological limitations that must be considered when interpreting the results and that define future research lines. The main constraint lies in the sample characteristics, which was reduced, predominantly female, and defined by strict exclusion criteria. This sample homogeneity compromises the external validity of the findings and their generalization to more heterogeneous populations, including individuals with lower educational levels (illiteracy), moderate/severe cognitive impairment, or motor and balance difficulties.
From an analytical perspective, although linear mixed models were used to control for covariates, the significant influence observed from sociodemographic variables such as age and educational level on cognitive performance constitutes a factor that moderates the interpretation of the pure intervention effect.
Regarding the training protocol, the low intensity and duration may have limited the statistical power to detect significant changes. Furthermore, the absence of long-term follow-up prevents the determination of the temporal persistence of the observed positive effects. Finally, the use of conventional assessment instruments, based on global scores, may not have captured all the subtle or specific changes induced by the multimodal MotoTiles intervention.
Future Directions
To optimize the impact of future research and strengthen empirical evidence, the following are recommended: Increase the sample size and ensure greater sociodemographic diversity to enhance external validity and the generalizability of results. Increase the frequency and/or duration of training sessions to determine the optimal dose required to generate significant effects. Incorporate a more exhaustive analysis of cognitive and motor reserve at baseline. This will allow for the use of more robust statistical models or designs that facilitate better group stratification and matching, more accurately isolating the causal effect of the MotoTiles intervention. Implement long-term follow-up to evaluate the stability and persistence of the training effects. Utilize more sensitive and specific measurement instruments that go beyond global scores to capture subtle changes in executive functions and kinematic parameters.
References
Arango-Lasprilla, J. C., Rivera, D., & Usuga, D. R. (2022). Neuropsicología en Colombia: Datos normativos, estado actual y retos a futuro. El Manual Moderno.
Arango-Lasprilla, J. C., Rivera, D., Aguayo, A., Rodríguez, W., Garza, M. T., Saracho, C. P., Rodríguez-Agudelo, Y., Aliaga, A., Weiler, G., Luna, M., Longoni, M., Ocampo-Barba, N., Galarza-del-Angel, J., Panyavin, I., Guerra, A., Esenarro, L., García de la Cadena, P., Martínez, C., & Perrin, P. B. (2015). Trail Making Test: Normative data for the Latin American Spanish speaking adult population. NeuroRehabilitation, 37(4), 639-661. https://doi.org/10.3233/nre-151284
Arokiaraj, A. S., Khairudin, R., & Sulaiman, W. S. W. (2020). The impact of a computerized cognitive training on healthy older adults: A systematic review focused on processing speed and attention. International Journal of Academic Research in Business and Social Sciences, 10(11), 645-685. https://doi.org/10.6007/IJARBSS/v10-i11/7647
Barlow, D. H. (2000). Unraveling the mysteries of anxiety and its disorders from the perspective of emotion theory. American Psychologist, 55(11), 1247. https://doi.org/10.1037/0003-066x.55.11.1247
Chan, A. T. C., Ip, R. T. F., Tran, J. Y. S., Chan, J. Y. C., & Tsoi, K. K. F. (2024). Computerized cognitive training for memory functions in mild cognitive impairment or dementia: A systematic review and meta-analysis. NPJ Digital Medicine, 7(1), 1-11. https://doi.org/10.1038/s41746-023-00987-5
Cohen, J. (1992). A power primer. Psychological Bulletin, 112(1), 155-159. https://doi.org/10.1037/0033-2909.112.1.155
Cruz-Peralta, M., & González-Celis, A. L. (2023). Intervenciones para mejorar la calidad de vida en adultos mayores: Revisión sistemática con preguntas PIO. Psicología y Salud, 33(2), 415-426. https://doi.org/10.25009/pys.v33i2.2824
Editverse. (2025). Comprensión de la corrección estadística: Bonferroni y más.
Eggenberger, P., Schumacher, V., Angst, M., Theill, N., & de Bruin, E. D. (2015). Does multicomponent physical exercise with simultaneous cognitive training boost cognitive performance in older adults? Clinical Interventions in Aging, 10, 1243-1259. https://doi.org/10.2147/CIA.S87732
Ehrari, H., Larsen, R. T., & Langberg, H. (2020). Effects of playful exercise in older adults on balance and physical activity: A randomized controlled trial. Population Ageing, 13, 207-222. https://doi.org/10.1007/s12062-020-09273-8
Entertainment Robotics. (2014). Clinical evidence of effects for Moto Tiles. https://www.Moto-tiles.com/effects.php
Escobar, M., Restrepo, M., & Uribe, L. (1999). Adaptación colombiana del Mini Mental State Examination (MMSE). Revista Colombiana de Psiquiatría, 28(2), 118-126. https://doi.org/10.1016/S0034-7450(99)00008-5
Feldberg, C., Stefani, D., Tartaglini, M. F., Hermida, P. D., García, L. M., Somale, M. V., & Allegri, R. (2020). La influencia de la educación y la complejidad laboral en el desempeño cognitivo de adultos mayores con deterioro cognitivo leve. Ciencias Psicológicas, 14(1), 1-19. https://doi.org/10.22235/cp.v14i1.2194
Hernández-Sampieri, R., & Mendoza, C. (2018). Metodología de la investigación: Las rutas cuantitativa, cualitativa y mixta. McGraw Hill México.
Jamovi. (2020). The jamovi project. https://www.jamovi.org
Jessen, J. D., & Lund, H. H. (2017). Study protocol: Effect of playful training on functional abilities in older adults: A randomized controlled trial. BMC Geriatrics, 17(1), 27. https://doi.org/10.1186/s12877-017-0416-5
Johnson, K., Lee, M., & White, R. (2019). Cognitive interventions and executive functions in older adults. Aging & Mental Health, 23(2), 234-245.
Knopman, D. S., Mosley, T. H., Catellier, D. J., & Coker, L. H. (2009). Fourteen-year longitudinal study of vascular risk factors, APOE genotype, and cognition: The ARIC MRI Study. Alzheimer’s & Dementia, 5(3), 207-214. https://doi.org/10.1016/j.jalz.2009.01.027
Liu, Y. X., Lund, H. H., & Wu, L. (2018). Playful cognitive training with physical interactive tiles for the elderly. In 2018 International Conference on Information and Communication Technology Robotics (ICT-ROBOT) (pp. 1-4). IEEE. https://doi.org/10.1109/ICT-ROBOT.2018.8549898
Lund, H. H. (2015). Play for the elderly – Effect studies of playful technology. In S. Bernhard (Ed.), Lecture Notes in Computer Science (Vol. 9194, pp. 500-511). Springer. https://doi.org/10.1007/978-3-319-20913-5_46
Lund, H. H., & Jessen, J. D. (2014). Effects of short-term training of community-dwelling elderly with modular interactive tiles. Games for Health Journal, 3(5), 289-295. https://doi.org/10.1089/g4h.2014.0028
Lund, H. H., Liu, Y.-X., & Leggieri, M. (2020a). Body and brain training for fall prevention. Journal of Robotics, Networking and Artificial Life, 7(3), 179-183. https://doi.org/10.2991/jrnal.k.200909.008
Lund, H. H., Liu, Y.-X., & Leggieri, M. (2020b). Body and brain training with big data and AI 2 – A pilot test of falls prevention. In Proceedings of the 2020 International Conference on Artificial Life and Robotics (pp. 10-13). ALife Robotics Co. https://doi.org/10.5954/ICAROB.2020.IS2-2
Ministerio de Salud. (Colombia). (1993). Resolución 8430 de 1993: Por la cual se establecen las normas científicas, técnicas y administrativas para la investigación en salud. https://acortar.link/QOT2C
Nasreddine, Z., Phillips, N., Bédirian, V., Charbonneau, S., Whitehead, V., & Collin, I. (2005). The Montreal Cognitive Assessment (MoCA): A brief screening tool for mild cognitive impairment. Journal of the American Geriatrics Society, 53(4), 695-699. https://doi.org/10.1111/j.1532-5415.2005.53221.x
National Institute for Aging. (2023, December 21). Memoria, olvido y envejecimiento. https://www.nia.nih.gov/espanol/memoria/memoria-olvido-envejecimiento
NeuronUP. (2024, November 26). ¿Cómo se explica el deterioro cognitivo de las personas de cincuenta años? https://acortar.link/WP1LKh
Osterrieth, P. A. (1944). Le test de copie d’une figure complexe: Contribution à l’étude de la perception et de la mémoire. Archives de Psychologie, 30, 206-356.
Pedraza, O. L., Salazar, A. M., Sierra, F. A., Soler, D., Castro, J., Castillo, P. C., Hernández, A., & Piñeros, C. (2016). Confiabilidad, validez de criterio y discriminante del Montreal Cognitive Assessment (MoCA) test, en un grupo de adultos de Bogotá. Acta Médica Colombiana, 41(4), 221-228. https://doi.org/10.36104/amc.2016.693
Peters, A. (2009). The effects of normal aging on myelin and nerve fibers: A review. Journal of Neurocytology, 36(5), 237-243. https://doi.org/10.1007/s11068-009-9026-2
Piech, J., & Czernicki, K. (2021). Rehabilitación de realidad virtual y exergames: Impacto físico y psicológico en la prevención de caídas entre las personas mayores: Una revisión de la literatura. Ciencias Aplicadas, 11(9), 4098. https://doi.org/10.3390/app11094098
Reitan, R. M., & Wolfson, D. (1985). The Halstead–Reitan Neuropsychological Test Battery: Therapy and clinical interpretation. Neuropsychological Press.
Rey, A. (1941). L’examen psychologique dans les cas d’encéphalopathie traumatique. Archives de Psychologie, 28, 286-340.
Salazar, A. M., & Maldonado, L. R. (2020). Desarrollo y validación del Cuestionario de Cambios Cognitivos (QCC). Psicogénero, 25(1), 1-17.
Salthouse, T. A. (2019). Trajectories of normal cognitive aging. Psychology and Aging, 34(1), 17-24. https://doi.org/10.1037/pag0000288
Silva-Fernandes, A., Cruz, S., Moreira, C. S., Pereira, D. R., Sousa, S. S., Sampaio, A., & Carvalho, J. (2022). Processing speed mediates the association between physical activity and executive functioning in elderly adults. Frontiers in Psychology, 13, 958535. https://doi.org/10.3389/fpsyg.2022.958535
Smith, A. (1973). Symbol Digit Modalities Test (SDMT) manual. Western Psychological Services.
Smith, J., Brown, K., & Taylor, M. (2020). Subjective measures and biases in cognitive assessment. Cognitive Science Review, 67(4), 345-356.
Torralva, T., Roca, M., Gleichgerrcht, E., López, P., & Manes, F. (2009). INECO Frontal Screening (IFS): A brief, sensitive, and specific tool to assess executive functions in dementia. Journal of the International Neuropsychological Society, 15(5), 777-786. https://doi.org/10.1017/S1355617709990415
UCLA Advanced Research Computing. (2025). Introduction to linear mixed models. https://stats.oarc.ucla.edu/other/mult-pkg/introduction-to-linear-mixed-models/
Wang, J., Fang, Y., Zhang, S., Qiu, Q., Liu, X., Li, X., Wu, L., & Yang, Y. (2021). Efectos de las baldosas MOTO sobre las funciones cognitivas y motoras en ancianos con deterioro cognitivo leve a moderado. Geriatría Práctica, 35(3), 261-264.
Zapata-Zabala, M., Cárdenas-Niño, L., & Cuartas-Arias, J. M. (2019). INECO Frontal Screening (IFS): Una herramienta psicométrica para evaluar la disfunción ejecutiva en policonsumidores. Suma Psicológica, 26(2), 119-126. https://doi.org/10.14349/sumapsi.2019.v26.n2.8
Funding: Funding was provided by Universidad El Bosque.
Data availability: The dataset supporting the results of this study is not available.
Conflict of interest: The authors declare that they have no conflicts of interest.
How to cite: Salazar, A. M., Bonilla, F. M., Carvajal Tavera, D. F., Castillo, M., Grosso, C., Jiménez, J., Romero, A. P., & Vargas, J. L. (2026). MotoTiles: A Tool for Cognitive and Motor Stimulation in Active Aging. Ciencias Psicológicas, 20(1), e-4723. https://doi.org/10.22235/cp.v20i1.4723
Authors’ contribution (CRediT Taxonomy): 1. Conceptualization; 2. Data curation; 3. Formal Analysis; 4. Funding acquisition; 5. Investigation; 6. Methodology; 7. Project administration; 8. Resources; 9. Software; 10. Supervision; 11. Validation; 12. Visualization; 13. Writing: original draft; 14. Writing: review & editing.
A. M. S. has contributed in 1, 2, 3, 4, 5, 6, 7, 10, 11, 12, 13, 14; F. M. B. in 1, 2, 3, 4, 5, 6, 7, 10, 11, 12, 13, 14; D. F. C. T. in 5, 6, 10, 13, 14; M. C. in 2, 5, 12; C. G. in 2, 5, 12; J. J. in 5; A. P. R. in 5; J. L. V. in 2, 5.
Scientific editor in-charge: Dr. Cecilia Cracco.
Ciencias Psicológicas; v20(1)
January - June 2026
10.22235/cp.v20i1.4723