10.22235/cp.v18i2.3285
Modelo híbrido de treinamento parental para mães de crianças pré-escolares com transtorno do espectro autista baseado na análise do comportamento aplicada para redução do estresse parental
Hybrid model of parent training for mothers of preschool children with autism spectrum disorder based on applied behavior analysis to reduce parental stress
Modelo híbrido de entrenamiento parental para madres de niños en edad preescolar con trastorno del espectro autista basado en el análisis de comportamiento aplicado para reducir el estrés parental
Aline Regina Emilio1, ORCID 0009-0007-1654-866X
João Rodrigo Maciel Portes2, ORCID 0000-0003-2512-4491
1 Universidade do Vale do Itajaí, Brasil, [email protected]
2 Universidade do Vale do Itajaí, Brasil
Resumo:
Este estudo buscou avaliar as contribuições de um treinamento parental híbrido realizado com oito mães de crianças pré-escolares com transtorno do espectro do autismo baseado na ciência da análise do comportamento aplicada para a redução do estresse parental. Foi realizado a construção e implementação do treinamento parental híbrido. A amostra foi dividida em grupo tratamento e controle. Em termos de análise de dados, foram feitas comparações do nível de estresse no período pré/pós-intervenção, assim como a análise de uma prática direta com a criança de forma presencial com o grupo tratamento. Os resultados obtidos demonstraram que as mães do grupo tratamento reagiram positivamente com as vídeos e materiais apresentados. No entanto, não foi observado diferenças estatísticas significativas para sugerir a redução do nível de estresse entre os dois grupos. As limitações do estudo foram o tamanho reduzido da amostra e o fato das crianças de ambos os grupos continuarem recebendo o tratamento em terapia intensiva durante a aplicação do treinamento parental.
Palavras-chave: autismo; treinamento de pais; telessaúde; análise do comportamento aplicada; estresse parental.
Abstract:
This study sought to evaluate the contributions of a hybrid parental training carried out with eight mothers of preschool children with autism spectrum disorder, based on the science of applied behavioral analysis for reducing parental stress. The hybrid parental training was constructed and implemented by the researchers. The sample was divided into two groups: a Treatment Group and a Control Group. In the data analysis, comparisons were made of the levels of stress pre- and post-intervention and for the treatment group, direct practice with the child in a face-to-face environment was also analyzed. The results showed that the mothers in the treatment group reacted positively to the video and materials presented; however, no significant statistical differences were found that would suggest a reduction in stress levels between the two groups as a result of the training given. The limitations of the study were its small sample size and the fact that the children in both groups continued to receive intensive therapy treatment during the application of the parental training.
Keywords: autism; parent training; telehealth; applied behavior analysis; parental stress.
Resumen:
Este estudio buscó evaluar los aportes de un entrenamiento parental híbrido realizado con ocho madres de niños preescolares con trastorno del espectro autista basado en la ciencia del análisis aplicado de la conducta para la reducción del estrés parental. Se llevó a cabo la construcción e implementación de un entrenamiento parental híbrido. Se dividió la muestra en grupo de tratamiento y control, y se realizaron comparaciones del nivel de estrés en el período pre/postintervención, así como el análisis de la práctica directa con el niño en un cara a cara con el grupo de tratamiento. Los resultados obtenidos demuestran que las madres del grupo de tratamiento reaccionaron positivamente a los videos y materiales presentados; sin embargo, no se observaron diferencias estadísticas significativas que sugieran una reducción en el nivel de estrés entre los dos grupos. Las limitaciones del estudio fueron el pequeño tamaño de la muestra y el hecho de que los niños de ambos grupos continuaron recibiendo tratamiento de terapia intensiva durante la implementación de la capacitación de los padres.
Palabras clave: autismo; formación de padres; telesalud; análisis aplicado del comportamiento; estrés parental.
Recebido: 10/03/2023
Aceito: 21/06/2024
As dificuldades apresentadas pelas crianças diagnosticadas com TEA não impactam apenas o individuo, mas também aqueles que convivem com elas, principalmente seus pais ou cuidadores (Dahiya et al., 2021). Pais de crianças com TEA enfrentam elevados níveis de estresse parental quando comparado aos pais de crianças com outras deficiências ou desenvolvimento típico (Craig et al., 2016). As crianças com TEA demandam de seus pais e cuidadores mais tempo e cuidados. Isto pode afetar diretamente toda vida dos envolvidos, e as mães geralmente são as que despendem mais tempo nesse cuidado, apresentando maior sobrecarga, e é comum elas renunciarem de sua vida pessoal e social para se dedicar aos cuidados de seu filho (Anjos & Morais, 2021; Portes & Vieira, 2022).
Uma estratégia para auxiliar os pais diante de seus desafios com filhos diagnosticados com TEA é a partir do treinamento parental, pois treinar os pais é uma alternativa promissora que oferece viabilidade, aceitabilidade e ótimo custo-benefício (Dawson-Squibb et al., 2020), além de que pode ser uma forma de reduzir a carga emocional e o estresse parental (Kurzrok et al., 2021; Sneed & Samelson, 2022). Geralmente os níveis de estresse parental em pais de crianças com TEA estão relacionados ao comportamento da criança, e/ou as barreiras de acesso à participação em atividades sociais, educacionais, e diante das preocupações a respeito dos tratamentos (Shepherd et al., 2018).
Pode-se definir o treinamento parental como uma estratégia que visa ensinar os pais a identificarem comportamentos disruptivos, analisar a função desses comportamentos, adotar estratégias para prevenção, bem como manejá-los e treinar a comunicação funcional. Dentre as principais técnicas destacam-se o uso do vídeo modelação, role-playing, instruções diretas através de aulas expositivas e materiais complementares (Wong et al., 2014).
Atualmente a análise do comportamento aplicada (Applied Behavioral Analysis, ABA), tem sido apontada com uma das principais ciências que tem contribuído significativamente com a intervenção precoce no TEA (Sella & Ribeiro, 2018). As intervenções sob este referencial teórico demonstram ser uma prática baseada em evidências para essa população (Steinbrenner et al., 2020; Virués-Ortega, 2010; Wong et al., 2015). Embora exista vasta literatura que apresenta evidências da eficácia do treino parental em famílias que tenham filhos diagnosticados com TEA baseados numa perspectiva da ABA (Lee & Meadan, 2020; Lopes et al., 2021; Nevill et al., 2018; Rahman et al., 2016; Wong et al., 2015), os impactos desses treinamentos sobre os indicadores de saúde mental são moderados e requerem maior produção científica sobre a temática (Mackenzie & Eack, 2022).
As famílias de crianças com TEA em localidades com baixos recursos encontram diversas barreiras como a qualificação dos profissionais, infraestrutura precária da saúde pública, alto custo dos serviços de saúde mental, a representação social sobre o transtorno na sociedade e a distância da sua residência e dos centros especializados (Dawson-Squibb et al., 2020; Viljoen et al., 2021). Diante disso, a implementação de treinamento parental para os pais de crianças com TEA por meio de tecnologias de informação e comunicação (TIC’s) envolvendo a teleprática podem favorecer o acesso a tratamentos baseados em evidências com baixo custo e a desenvolver habilidades sociais e de comunicação das crianças com TEA (Camden et al., 2019; Parsons et al., 2017; Wilkes-Gillan & Lincoln, 2018). Apesar da escassez de aplicações em tecnologias para crianças com deficiências, os estudos disponíveis relatam resultados promissores para crianças com TEA (Samadi et al., 2020; Vismara et al., 2018).
A teleprática é um termo geral que contempla outros termos, como telessaúde e telemedicina, e pode ser definida como uma forma de prestar serviços profissionais à distância através do uso da internet (Meadan et al., 2022). A teleprática pode ser oferecida em duas modalidades, assíncrona e síncrona. A primeira pode ser definida quando as informações, como vídeos, fotos, ou arquivos de áudio são gravados e trocados via tecnologia entre o terapeuta e o cliente sem interação ao vivo entre eles e a segunda é quando há a interação em tempo real através das TIC’s. Quando os métodos síncronos e assíncronos são usados em combinação, isso é chamado de teleprática híbrida, que combina os benefícios das abordagens síncrona e assíncrona (Dudding, 2013). Entende-se também como modelo híbrido, a combinação das estratégias de teleprática com o ensino presencial, que foi a modalidade adotada nessa pesquisa.
A partir desse panorama o presente estudo teve como objetivo avaliar as contribuições de um modelo híbrido de treinamento parental para mães de crianças pré-escolares com TEA baseado na ABA para redução do estresse parental.
Método
O presente estudo caracteriza-se como ensaio clínico não randomizado (quase-experimental), ele é um recorte de uma pesquisa de dissertação de mestrado aprovada pelo Comitê de Ética da Universidade do Vale do Itajaí na data de 25/04/2022 e sob o no. 5.366.120. Nesse tipo de ensaio clínico, controla-se a exposição das variáveis independentes diante dos participantes, e os grupos não apresentam randomização entre eles (Hernández-Sampieri et al., 2013).
Participantes
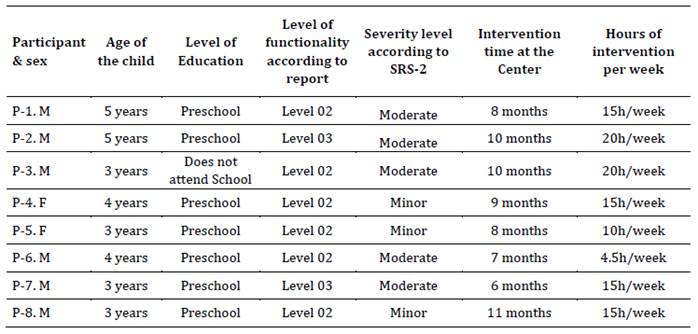
A amostra desta pesquisa se deu por conveniência, sendo que participaram do estudo oito mães, variando entre 34 e 44 anos de idade, e seus filhos com média de idade de 3,75 com TEA. Essas crianças realizavam intervenção em um núcleo de intervenção comportamental em uma cidade localizada no sul do Brasil, aproximadamente a 8 meses. Maiores informações foram apresentadas na Tabela 1 (caracterização da amostra) e na Tabela 2 (dados dos filhos da amostra).
Instrumentos
Questionário sociodemográfico: instrumento construído pelos pesquisadores, que buscou levantar informações a respeito das crianças e mães participantes, como gênero, idade, ano do diagnóstico, situação escolar e tempo em que a criança está em intervenção ao todo e o tempo específico no Núcleo, e para as mães buscou entender qual a naturalidade, estado civil, escolaridade, profissão, renda familiar, quantidade de filhos, membros que moram na mesma residência, cuidadores da criança, e se fazia acompanhamento psicológico.
Checklist de videoconferência: documento criado pelos pesquisadores para ser utilizado como um roteiro durante as videoconferências realizadas com as mães do grupo tratamento, para seguir uma padronização. Nele constavam lembretes como não ultrapassar o tempo de 10 minutos durante a videoconferência, diretrizes para como conduzir esse momento e que informações eram necessárias colher.
Roteiro de treinamento prático presencial: foi totalmente criado pelos pesquisadores com o objetivo de que no momento do encontro presencial pudessem observar as habilidades das participantes que ensinadas durante os vídeos. O documento apresentava uma sequência de solicitações que a pesquisadora realizou para as participantes. Conforme cada solicitação era executada ou não pela participante, a pesquisadora realizava a próxima ou a auxiliava a executar. As solicitações eram oportunidades de ensino referente aos conteúdos dos vídeos para que as participantes realizassem com a criança. Foram abordadas habilidades de engajamento da criança, motivação, reforço, instrução, economia de fichas, tipos e ajuda, ensino incidental e por tentativas discretas, função de comportamento, manejo de comportamento inadequado, e imitação. Também foi incluído neste documento condutas para a pesquisadora realizar caso a criança apresente comportamento inadequado.
Protocolo de observação do treinamento prático presencial: foi um protocolo totalmente criado pelos autores com questões fechadas em uma escala tipo Likert na qual os observadores puderam analisar o desempenho das mães nos vídeos do treinamento prático presencial. Este documente estava relacionado com o Roteiro de treinamento prático presencial, pois foi assim foi possível avaliar se participantes diante das solicitações da pesquisadora conseguiram ou não realizar, assim como se as fizeram de foram independentes, ou necessitaram de algum tipo de ajuda da pesquisadora (modelação ou verbal.
Escala de Responsividade Social (SRS-2): é uma escala Likert composta por
diferentes formulários para diferentes faixa etárias que busca quantificar de
forma quantitativa e confiável uma ampla gama de possíveis prejuízos de
socialização, comunicação, comportamentos repetitivos e interesses restritos
que possam estar associados ao TEA e apresentar os níveis dos sintomas entre
leve, moderado e severo, por meio das respostas preenchidas por pais ou
professores, é composta por 65 itens mensurando (Constantino & Gruber,
2020). Os estudos de
validação para o contexto brasileiro desta escala demonstram propriedades
psicométricas com valores de consistência ![]() = 0,95 e
= 0,95 e ![]() = 0,97, sensibilidade de 96,8 %, especificidade de
100% e valor preditivo negativo de 99,99 % para identificação de TEA
(Borges & Hauck-Filho, 2020).
= 0,97, sensibilidade de 96,8 %, especificidade de
100% e valor preditivo negativo de 99,99 % para identificação de TEA
(Borges & Hauck-Filho, 2020).
Escala de Estresse Parental – Versão Reduzida: Para avaliar o estresse parental, foi utilização a adaptação portuguesa em sua versão reduzia da Escala de Estresse Parental – Versão reduzida (PSI -SF) que possui 36 itens e é dividida em três subescalas: criança difícil; sofrimento parental; interações disfuncionais (Santos, 2008). No estudo de validação da PSI-SF em Portugal (Santos, 2008), apresenta propriedades psicométricas com valor do coeficiente alfa de Cronbach foi de 0,92. Entretanto, o instrumento ainda não possui validação para o contexto brasileiro, mas devido a aproximação linguística entre Brasil e Portugal optou-se pela utilização desta escala, e tendo em vista a escassez de instrumentos para avaliar essa demanda validados para território brasileiro.
Procedimentos
Treinamento Parental Híbrido
A construção da proposta do treinamento parental para os pais de crianças com TEA seguiu algumas etapas: a) discussão entre os pesquisadores sobre treinamento parental no formato híbrido para pais/cuidadores de crianças pré-escolares diagnosticadas com TEA, b) revisão da literatura dos últimos cinco anos a respeito da temática, c) definição dos conteúdos de cada vídeo, d) preparação do material visual (slides) para apresentar nos vídeos, gravação e edição dos vídeos, e) verificação e correção dos vídeos, f) disponibilização dos vídeos, g) aplicação do treinamento parental, e h) avaliação da eficácia.
Os temas abordados durante o treinamento foram: 1) o que é Transtorno do Espectro do Autismo e a ABA utilizada com essa demanda, 2) princípios básicos como reforço, punição, extinção, entre outros, 3) o que é comportamento, como defini-lo e suas possíveis funções, 4) como estabelecer operação motivadora e realizar uma avaliação de preferência com a criança, 5) sistemas de ajuda no ensino de habilidades (sistema de dicas) e como apresentar instruções de forma clara e se necessário o redirecionamento de comportamento, 6) estratégias de reforçamento diferencial aplicada no dia a dia, 7) a importância do brincar e possibilidades de brincar e ensinar com a criança, 8) como montar e realizar com a criança um cronograma de atividades, e importância e como estabelecer o controle instrucional, 9) a diferença entre ensino naturalístico e estruturado, e como aplica-los.
Nos vídeos eram apresentados exemplos e relação prática com o dia a dia, com linguagem clara e relacionando os termos técnicos com termos acessíveis para as mães. Cada vídeo teve aproximadamente 40 minutos. Os vídeos de temas de 1 a 6 foram compostas de duas vídeos e os demais apenas um, e todos disponibilizados via YouTube em um link privado. Durante todo o treinamento as mães do grupo tratamento continuavam tendo acesso a todos os vídeos já assistidos.
Coleta de dados
Primeira etapa
Inicialmente a pesquisadora enviou um convite via WhatsApp para os responsáveis pelas crianças que eram atendidas no Núcleo os convidando para participarem da pesquisa. Conforme as mães aceitavam o convite (respondendo a mensagem), e estavam de acordo com os critérios de inclusão para este estudo foram: o filho apresentou diagnóstico de TEA entre níveis de sintomas de leve a grave compatíveis com a Escala de Responsividade Social (SRS-2); a criança estava em intervenção precoce no Núcleo dentro de um período de 6 a 12 meses; tinha entre 2 anos e 6 meses a 6 anos; as participantes nunca realizaram treinamento ou cursos a respeito da análise do comportamento aplicada; tinham acesso a internet; eram alfabetizados; tinham disponibilidade de tempo para comparecer ao núcleo. Os critérios de exclusão: se apresentasse qualquer deficiência ou transtorno na área do neurodesenvolvimento que pudesse impedir de assistir e participar das aulas do treinamento ou de responder os instrumentos.
Era realizada a divisão dos grupos de forma randomizada, sendo que para as quatro primeiras mães que aceitaram participar da pesquisa compuseram o Grupo Tratamento, e as demais o Grupo Controle, e posteriormente foi agendado um horário no qual a participante compareceu no Núcleo e foi disponibilizado o Termo de Consentimento Livre e Esclarecido para o Grupo Tratamento e no Grupo Controle, em seguida foi aplicado o questionário sociodemográfico, o SRS-2, e o Índice de Estresse Parental (PSI). Nesse encontro, apenas as mães do Grupo Tratamento, receberam instruções pela pesquisadora sobre o processo do programa, como acessar os vídeos (de aproximadamente 30/40 minutos cada), de diferentes temas a respeito do TEA e ABA.
Iniciou o treinamento disponibilizados dois vídeos de dois módulos por semana para que fossem assistidos em até 7 dias, e após assistirem foi agendada e realizado uma videoconferência com a pesquisadora, posterior a isso mais duas módulos foram disponibilizados. Entretanto, algumas mães não conseguiram realizar dentro do prazo estabelecido, e foi necessário disponibilizar um módulo com o prazo de 15 dias para assistirem e realizar a videoconferência. E assim ocorreu até o último momento que foi o encontro presencial no qual se realizou a parte prática, que foi gravada para a análise das juízas. Todo esse processo ocorreu durante 13 semanas.
E para as quatro participantes do Grupo Controle foi realizado um acolhimento das demandas pela pesquisadora e instruído que os participantes iriam receber mensagens via telefone (WhatsApp) para o acompanhamento do caso, e aqueles que informaram alguma demanda, esta seria encaminhada para a equipe técnica responsável pelo atendimento da criança no Núcleo, e quando finalizasse a pesquisa receberiam o mesmo treinamento.
Segunda etapa
Após primeira etapa, as mães assistiram os dois primeiros vídeos, e realizaram videoconferência. Durante a videoconferência dos participantes do Grupo de Tratamento foi administrado o checklist de videoconferência e liberado os próximos vídeos. E esta etapa foi repetida de forma quinzenal até que as participantes terminaram de assistir os vídeos e então agendaram o encontro presencial para realizar a parte prática do treinamento.
Terceira etapa
Na terceira etapa de coleta de dados, a pesquisadora e as participantes do Grupo Tratamento compareceram de forma individual com seus filhos ao Núcleo e realizaram a parte prática do treinamento que foi gravada para realização da observação dos juízes.
O encontro ocorreu em uma sala de atendimento que era equipada com duas câmeras que realizam captura de áudio e vídeo. Foi realizada uma sessão de no máximo 20 minutos, seguindo o roteiro de treinamento prático presencial. Ao finalizar a sessão a participante foi encaminhada para outra sala em que foi aplicado novamente o Índice de Estresse Parental-Versão Reduzida (PSI-SF).
Quarta etapa
Dois juízes com formação e experiência em ABA, que atuavam no Núcleo de Intervenção que ocorreu a pesquisa, realizaram a análise de forma independente dos quatro vídeos gravados dos encontros presenciais práticos que foram realizados com as participantes do Grupo Tratamento. E para a análise seguiram o protocolo de observação do treinamento prático presencial.
Análise dos dados
Primeiramente as informações coletadas através do questionário sociodemográfico foram organizadas, tabuladas e analisadas, de forma descritiva, com o objetivo de caracterizar o perfil das participantes quanto aos objetivos desta pesquisa.
Os dados obtidos na escala Índice de Estresse Parental – Versão Reduzida (PSI-SF) foram analisados por meio de estatísticas descritivas, na qual buscou-se descrever um conjunto de dados, como também por meio de estatística inferencial como uma maneira de compreender, comparar e fazer conclusões sobre os dados apresentados pelos participantes da pesquisa nos instrumentos utilizados (Dancey & Reidy, 2019). Foram usados os testes não paramétricos Wilcoxon para avaliar as diferenças intragrupos e teste de Mann Whitney para analisar as diferenças entre Grupo tratamento e Grupo controle (Dancey & Reidy, 2019).
Os vídeos gravados do treinamento presencial com os participantes foram analisados individualmente em um segundo momento, através do protocolo de observação do treinamento prático presencial, no qual foi contabilizado a ocorrência de cada item deste instrumento durante o treinamento. Os 3 primeiros minutos dos vídeos foram desconsiderados da análise, por se tratar de um momento em que as participantes e as crianças estavam se adaptando com a sala de atendimento, e o tempo restante foi codificado.
Para a verificar da fidedignidade do instrumento de observação do comportamento dos participantes durante o treinamento, foi utilizado a análise de dois juízes especialistas e experientes em ABA há mais de 02 anos. Eles foram orientados sobre a utilização do protocolo de observação do treinamento prático presencial, assistiram de forma individual os vídeos, e através do protocolo identificaram se as participantes conseguiram apresentar ou não os comportamentos solicitados pela pesquisadora. E nos itens que apresentaram divergência a pesquisadora atuou como terceira juíza e analisou os itens para concluir a análise.
Em geral o índice de concordância satisfatório deve ser no mínimo 80 % entre os observadores, e para que se obter o índice de concordância foi utilizada a seguinte fórmula: ∑A/ ∑(A+D) x 100 após a análise de cada vídeos de cada juíza. Como resultado da análise de juízes, obteve-se um índice médio geral de 95,45 %.
Resultados e Discussão
Ao analisar os dados demográficos das participantes (Tabela 1), constatou-se que todas mantinham relação conjugal com o pai da criança e moravam juntos, assim como o alto nível de escolaridade, sendo que 07 delas possuíam uma graduação ou pós-graduação, apenas a participante P-3 possuía ensino médio completo. E referente a renda familiar, eram superiores a R$ 4.001,00 reais, tendo participantes com renda superior a R$ 7.000,00 reais. Esses dados tendem a contribuem para que as mães tenham maior acesso a informação sobre autismo e intervenção de qualidade, o que sugere menores níveis de estresse parental, pois fatores transversais além do TEA, como conflitos no relacionamento conjugal, falta de rede de apoio, falta de políticas públicas para garantir o atendimento a criança com TEA, baixo nível socioeconômico e de escolaridade contribuem negativamente com a saúde mental dos familiares (Anjos & Morais, 2021).
Ainda sobre as informações das participantes, foi possível observar que apenas a participante P-1, não estava no mercado de trabalho no momento da pesquisa.
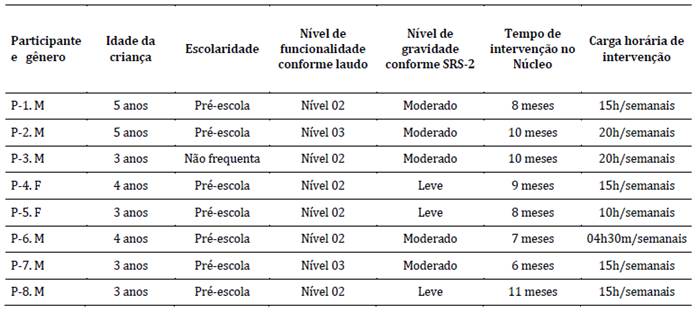
Referente aos resultados da escala SRS-2 (Tabela 2), que avaliou o nível de suporte das crianças por meio das respostas das mães, apresentou que 03 das 08 crianças, são compatíveis com nível leve de suporte, e as demais com nível moderado. E através da literatura já existente é possível constatar que quanto maior o nível de suporte que a criança necessite, a manifestação de sintomas é mais elevada, e pode ter relação com o estresse parental (Hartley et al., 2017).
Foi observado que a participante P-5 do Grupo Controle apresentou os menores escores de estresse na escala (escore pré-teste 67/pós-teste 73), entretanto, este foi o único caso que a participante da pesquisa não era o principal cuidador da criança, pois era o pai (que não participou da pesquisa), e outra dado, é que a mãe desde o diagnóstico da criança se manteve no mercado de trabalho, enquanto o pai se dedicou aos cuidados da criança. Geralmente a figura paterna não é o cuidador principal do filho com TEA e não se envolve em atividades de cuidados básicos (Jorge et al., 2021).
Tabela 1: Caracterização da amostra (N = 8)
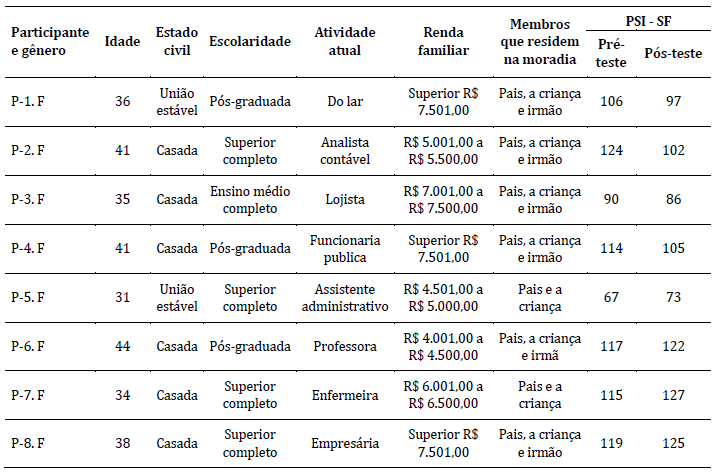
Tabela 2: Caracterização dos filhos da amostra (N = 8)
Nota: F: feminino; M: masculino
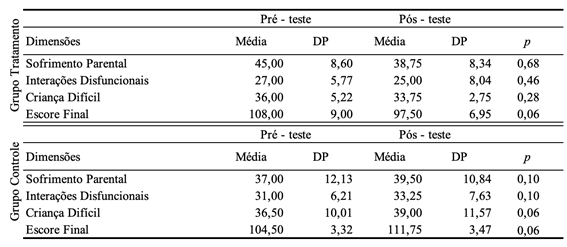
Os resultados obtidos pela escala PSI-SF, foram tabulados em uma planilha do Excel e realizado cálculos para se obter a média e desfio padrão por participante, e de grupo, tanto no pré-intervenção e no pós-intervenção. Além disso, foi utilizado os testes não paramétricos de Wilcoxon para realizar a comparação dos grupos nos dois momentos da pesquisa (pré e pós), e esses dados foram apresentados na Tabela 3. E para a comparação dos resultados entres grupos foi utilizado o Mann-Whitney.
Tabela 3: Resultado do pré/pós-teste PSI-SF
A pesquisa envolveu 8 participantes, todas do sexo feminino, com média de idade de 37,5 anos, todas mães das crianças diagnosticadas com TEA em idade pré-escolar, sendo que já é esperado que a mãe seja o familiar que assuma o papel de principal cuidar (Machado et al., 2018), o que vem de encontro com está pesquisa. Diante disto, é comum que elas apresentem sobrecarga, falta de apoio, questões de saúde, impacto em suas vidas e relações, e isto foi avaliado através da dimensão Sofrimento Parental da PSI-SF.
Nesta dimensão inicialmente foi comparada os escores das participantes do mesmo grupo nos dois momentos (pré/pós), e ambos os grupos não apresentaram diferenças estatísticas significativas (p < 0), e nas comparações das médias entre grupos nesta mesma dimensão, no pré-teste a média do grupo tratamento M = 45,00 (DP = 8,60), sendo maior que a média do grupo controle M = 37,00 (DP = 12,130, o pós-teste a médio do grupo tratamento foi de M = 38,75 (DP = 8,34), dessa forma, a média diminuiu e passou a ser menor que a do grupo controle que foi de M = 39,50, sendo assim, aumentou no pós-teste. Apesar disso, não houve diferença esteticamente significativa entre os dois grupos (U = 0,48; p < 0).
Colaborando com Sofrimento Parental, algumas pesquisas sugerem que as mães de crianças com TEA sofrem maiores impactos em suas vidas, sendo em sua saúde física, mental e/ou profissional, devido a necessidade de cuidado intensivo que o filho apresenta, e gerando sentimento de sobrecarga (Machado et al. 2018).
Na dimensão de Interações Disfuncionais, é avaliado as expectativas dos pais sobre o relacionamento estabelecido com a criança, a possibilidade de serem reforçados, aceitos, o estabelecimento de vínculo com seu filho, ou seja, o nível de satisfação relacional com a criança. Ao ser comparado o resultado das participantes do mesmo grupo, não houve mudança considerada significativa (p < 0), e o mesmo ocorreu quando realizada a comparação dos entre grupos (U = 1; p < 0), este resultado revela que o sentimento de incapacidade das mães em construir um relacionamento próximo com seus filhos diagnosticados com TEA pode vir a ameaçar a própria concepção de identidade da mãe e contribuir para o estresse materno (Porter & Loveland, 2019), e ao aumentar a interação entre pais e filhos, assim como o sentimento de estarem conectados, pode contribuir para redução do nível estresse (Anjos & Moraes, 2021).
A última dimensão é nomeada como Criança Difícil, e suas afirmações estão relacionadas as características do filho, como humor, hiperatividade, exigência, adaptabilidade, aceitação, autonomia, e o quanto estas características impactam na vida dos pais. Na comparação intragrupo, não foram obtidos resultados com significância estatística (p < 0), e quando comparado o resultado de ambos os grupos (U = 1; p < 0), quanto no pós-teste (U = 0,68), sugerindo que a percepção a respeitos dos filhos e de seus comportamentos para a amostra dos dois grupos são parecidas, e esses resultados corroboram que existe ligação do estresse das mães com à gravidade dos sintomias centrais de seus filhos com TEA, e a literatura indica forte relação entre o estresse parental e as características/sintomatologia do TEA (Siu et al., 2019; Tsermentseli & Kouklari, 2021).
Na somatória das dimensões (Escore final), e na análise entre as participantes do grupo tratamento, novamente não foi possível constatar relevância estatística (p < 0). Quando comparado as médias do escore final nos dois momentos, no pré-teste o grupo tratamento apresentou M = 108,00 (DP = 9,00), sendo maior que a do grupo controle M = 104,50 (DP = 3,32), entretanto no pós-teste realizado logo após o treinamento parental, o grupo tratamento reduzido a média do escore final para M = 97,50 (DP = 6,95), enquanto o grupo controle aumentou para M = 111,75 (DP = 3,47). E entre os grupos (U = 0,68; p < 0) e do pós-teste (U = 0,34; p < 0) o que não sugeriu significância, com isso foi possível concluir que não houve diferenças que pudessem sugerir que a participação do grupo tratamento no treinamento parental híbrido impactou significativamente no nível de estresse, quando realizadas as comparações por meio de análise estatística.
Esta pesquisa, assim como outras sobre treinamento parental também não apresentaram evidências que apoiem uma mudança significativa no estresse parental nessa população (Dai et al., 2018; Fisher et al., 2020; Mackenzie & Eack, 2022). E isto pode estar associado ao fato das crianças se encontravam em intervenção e as participantes estavam assistidas por profissionais especialistas em TEA, ou que o estresse é influenciado por diferentes variáveis, como característica da própria pessoa, características da criança, estrutura e funcionamento familiar, vínculo estabelecido, fatores sociais e socioeconômicos, rede de apoio, capacidade de acesso a informação e intervenção de qualidade, contexto cultural, entre outros (Louie et al., 2017) e para afirmar que o treinamento parental é suficiente para reduzi-lo, existe a necessidade de contemplar essas variáveis em investigações futuras.
Cabe ressaltar a importância de instrumentalizar e empoderar pais e cuidadores de crianças com TEA, e apesar da ausência de dados estatísticos, a amostra do grupo tratamento apresentaram opiniões positivos, como que a partir do treinamento que técnicas ensinadas podem ser introduzidas em suas rotinas, que o conteúdo era interessante e necessário, e que as auxiliaria em diferentes aspectos, como o manejo de comportamentos disruptivos, generalização e ensino de novas habilidades. Isto contribui diretamente para o desenvolvimento da criança e melhora no contexto familiar, e ao ampliar a compreensão a respeito de todo processo que envolve o TEA, pode contribuir com melhora significativa não só nos níveis de estresse parental, mas também em níveis de ansiedade, depressão e esperança das mães (Liu et al. 2021).
Considerações finais
Essa pesquisa teve como principal objetivo avaliar as contribuições de um modelo híbrido de treinamento parental para mães de crianças pré-escolares com TEA baseado na ABA para redução de estresse parental. Conclui-se após as falas das participantes do grupo tratamento, a importância e contribuição do que foi ensinado para suas rotinas, assim como, foi observado que na prática junto com a pesquisadora, as participantes conseguiram implementar técnicas adequadamente, sendo estes resultados qualitativos da pesquisa. Embora não seja possível afirmar que houve uma redução do estresse parental quando comparados os grupos de tratamento e controle.
Oportunizar as mães de crianças com TEA um modelo de treinamento parental sob os princípios da ABA pode auxiliar em conscientizá-las que são capazes de contribuir com o desenvolvimento de seus filhos, perceberem que existe maneiras efetivas de ensinar novas habilidades ou de manejar comportamento disruptivos, ampliar o seu conhecimento e também minimizar o impacto do estresse parental, inclusive é indicado a aplicação desse treinamento com outros cuidadores para avaliar os seus efeitos relacionados ao estresse parental nesses atores. Atualmente o treinamento parental se mostra uma ferramenta de baixo custo, e no formato híbrido, torna-se mais acessível as famílias.
Contudo, ressalta-se que o estudo apresentou limitações, destaca-se uma amostra restrita (N = 8) o que comprometeu significativamente a validade dos achados, e que as mães acompanham seus filhos em uma instituição especializada e particular. Além disso, não foi investigado de modo minucioso outras variáveis que pudessem contribuir para a comparação do estresse pré/pós-intervenção, por exemplo relação conjugal, saúde mental materna, demanda dos demais filhos, sua percepção a respeito do filho com TEA, entre outras. Identificamos também como uma dificuldade, o fato de a pesquisadora já ter tido oportunidade anterior em atender as crianças que compunha a amostra, e apresentar controle instrucional com elas, o que pode ter sido um estímulo para que elas apresentassem o comportamento esperado durante o treinamento presencial prático. Ademais, o fato de as crianças estarem em atendimento no núcleo de forma intensiva e regular baseada em ABA, se tornou uma variável interveniente.
Diante do exposto, sugere-se a replicação desta pesquisa levando em consideração as mudanças necessárias relacionadas as limitações apresentadas, para que assim, se possa tentar obter melhores resultados.
Referências:
American Psychiatric Association. (2023). DSM-5TR: Manual diagnóstico e estatístico de transtornos mentais (5ª ed. Revisado). Artmed.
Anjos, B. B., & Morais, N. A. (2021). As experiências de famílias com filhos autistas: uma revisão integrativa da literatura. Ciências Psicológicas, 15(1), e2347. https://doi.org/10.22235/cp.v15i1.2347
Borges, L. & Hauck-Filho, N. (2020). Escala de Responsividade Social (SRS-2). Hogrefe.
Camden, C., Pratte, G., Fallon, F., Couture, M., Berbari, J., & Tousignant, M. (2020). Diversity of practices in telerehabilitation for children with disabilities and effective intervention characteristics: results from a systematic review. Disability and rehabilitation, 42(24), 3424-3436. https://doi.org/10.1080/09638288.2019.1595750
Centers for Disease Control and Prevention. (2023). CDC Launches Autism Data Visualization Tool to Improve Access to Data. https://www.cdc.gov/ncbddd/autism/index.html
Constantino, J. N., & Gruber C. P. (2020). SRS II: Escala de Responsividade Social. Hogrefe.
Craig, F., Operto, F. F., De Giacomo, A., Margari, L., Frolli, A., Conson, M., Ivagnes, S., Monaco, M., & Margari, F. (2016). Parenting stress among parents of children with Neurodevelopmental Disorders. Psychiatry Research, 242, 121-129. https://doi.org/10.1016/j.psychres.2016.05.016
Dahiya, A. V., Openden, D., Ostmeyer, K. F., Anderson, R. M., & Scarpa, A. (2021). Pivotal response treatment for autism: A brief report on training for rural communities. Journal of Community Psychology, 49(7), 2983-2994. https://doi.org/10.1002/jcop.22558
Dai, Y. G., Brennan, L., Como, A., Hughes-Lika, J., Dumont-Mathieu, T., Rathwell, I. C., Minxhozi, O., Aliaj, B., & Fein, D. A. (2018). A video parent-training program for families of children with autism spectrum disorder in Albania. Research in autism spectrum disorders, 56, 36-49. https://doi.org/10.1016/j.rasd.2018.08.008
Dancey, C., & Reidy, J. (2018). Estatística Sem Matemática para Psicologia. Penso.
Dawson-Squibb, J. J., Davids, E. L., Harrison, A. J., Molony, M. A., & de Vries, P. J. (2020). Parent education and training for autism spectrum disorders: Scoping the evidence. Autism: the international journal of research and practice, 24(1), 7-25. https://doi.org/10.1177/1362361319841739
Dudding, C. (2013). Reimbursement and telepractice. Perspectives on Telepractice, 3, 35-40. https://doi.org/10.1044/teles3.2.35
Fisher, W. W., Luczynski, K. C., Blowers, A. P., Vosters, M. E., Pisman, M. D., Craig, A. R., Hood, S. A., Machado, M. A., Lesser, A. D., & Piazza, C. C. (2020). A randomized clinical trial of a virtual-training program for teaching applied-behavior-analysis skills to parents of children with autism spectrum disorder. Journal of Applied Behavior Analysis, 53(4), 1856-1875. https://doi.org/10.1002/jaba.778
Hartley, S. L., Papp, L. M., Mihaila, I., Bussanich, P. M., Goetz, G., & Hickey, E. J. (2017). Couple conflict in parents of children with versus without Autism: self- reported and observed findings. Journal of Child and Family Studies, 26(8), 2152-2165. https://doi.org/10.1007/s10826-017-0737-1
Hernández-Sampieri, R., Fernández-Collado, C., & Baptista Lucio, P. (2013). Metodologia da Pesquisa (5a ed.). Penso.
Jorge, G. H., Santos, Y. L. C. M., Portes, J. R. M., & Bossardi, C. N. (2021). Envolvimento paterno de pais de crianças com o Transtorno do Espectro Autista. Boletim - Academia Paulista de Psicologia, 41(101), 175-184. https://doi.org/10.5935/2176-3038.20210018
Kurzrok, J., McBride, E., & Grossman, R. B. (2021). Autism-specific parenting self-efficacy: An examination of the role of parent-reported intervention involvement, satisfaction with intervention-related training, and caregiver burden. Autism: the international journal of research and practice, 25(5), 1395-1408. https://doi.org/10.1177/1362361321990931
Lee, J. D., & Meadan, H. (2020). Parent-mediated interventions for children with ASD in low-resource settings: a scoping review. Review Journal of Autism and Developmental Disorders, 8(3), 285-298. https://doi.org/10.1007/s40489-020-00218-7
Liu, G., Wang, S., Liao, J., Ou, P., Huang, L., Xie, N., He, Y., Lin, J., He, H. G., & Hu, R. (2021). The efficacy of WeChat-Based Parenting Training on the psychological well-being of mothers with children with autism during the COVID-19 pandemic: quasi-experimental study. JMIR Mental Health, 8(2), e23917. https://doi.org/10.2196/23917
Lopes, V. D., Murari, S. C., & Kienen, N. (2021). Capacitação de pais de crianças com TEA: revisão sistemática sob o referencial da Análise do Comportamento. Revista Educação Especial, 34, e19, 1-28. https://doi.org/10.5902/1984686X43768
Louie, A. D., Cromer, L. D., & Berry, J. O. (2017). Assessing parenting stress: Review of the use and interpretation of the Parental Stress Scale. The Family Journal, 25(4), 359-367. https://doi.org/10.1177/1066480717731347
Machado, M. S., Londero, A. D., & Pereira, C. R. R. (2018). Tornar-se família de uma criança com transtorno do espectro autista. Contextos Clínicos, 11(3), 335-350. https://dx.doi.org/10.4013/ctc.2018.113.05
Mackenzie, K. T., & Eack, S. M. (2022). Interventions to improve outcomes for parents of children with autism spectrum disorder: a meta-analysis. Journal of Autism and Developmental Disorders, 52, 2859-2883. https://doi.org/10.1007/s10803-021-05164-9
Meadan, H., Lee, J. D., & Chung, M. Y. (2022). Parent-implemented interventions via telepractice in autism research: A review of social validity assessments. Current Developmental Disorders Reports, 9(4), 213-219. https://10.1007/s40474-022-00259-z
Nevill, R. E., Lecavalier, L., & Stratis, E. A. (2018). Meta-analysis of parent-mediated interventions for young children with autism spectrum disorder. Autism: the international journal of research and practice, 22(2), 84-98. https://doi.org/10.1177/1362361316677838
Parsons, D., Cordier, R., Vaz, S., & Lee, H. (2017). Parent-mediated intervention training delivered remotely for children with autism spectrum disorder living outside of urban areas: systematic review. Journal of Medical Internet Research, 19(8), e198. https://doi.org/10.2196/jmir.6651
Porter, N., & Loveland, K. A. (2019). An integrative review of parenting stress in mothers of children with autism in Japan. International Journal of Disability, Development and Education, 66(3), 249-272. https://doi.org/10.1080/1034912X.2018.1439159
Portes, J. R. M., & Vieira, M. L. (2022). Percepção parental sobre o filho com autismo: as repercussões na adaptação familiar. Revista Psicologia em Pesquisa, 16(2), 1-23. http://dx.doi.org/10.34019/1982-1247.2022.v16.32614
Rahman, A., Divan, G., Hamdani, S. U., Vajaratkar, V., Taylor, C., Leadbitter, K., Aldred, C., Minhas, A., Cardozo, P., Emsley, R., Patel, V., & Green, J. (2016). Effectiveness of the parent-mediated intervention for children with autism spectrum disorder in south Asia in India and Pakistan (PASS): a randomised controlled trial. The Lancet. Psychiatry, 3(2), 128-136. https://doi.org/10.1016/S2215-0366(15)00388-0
Samadi, S. A., Bakhshalizadeh-Moradi, S., Khandani, F., Foladgar, M., Poursaid-Mohammad, M., & McConkey, R. (2020). Using hybrid telepractice for supporting parents of children with ASD during the COVID-19 lockdown: A feasibility study in Iran. Brain Sciences, 10(11), 892. https://doi.org/10.3390/brainsci10110892
Santos, S. V. (2008). Forma reduzada do parenting stress index (PSI): Estudo Preliminar. XII Conferência Internacional Avaliação, Formas e Contextos.
Sella, A. C., & Ribeiro, D. M. (2018). Análise do comportamento aplicada ao transtorno do espectro autista. Appros Editora e Livraria Eireli-ME.
Shepherd, D., Landon, J., Taylor, S., & Goedeke, S. (2018). Coping and care-related stress in parents of a child with autism spectrum disorder. Anxiety, Stress, and Coping, 31(3), 277-290. https://doi.org/10.1080/10615806.2018.1442614
Siu, Q. K., Yi, H., Chan, R. C., Chio, F. H., Chan, D. F., & Mak, W. W. (2019). The role of child problem behaviors in autism spectrum symptoms and parenting stress: A primary school-based study. Journal of Autism and Developmental Disorders, 49, 857-870. https://doi.org/10.1007/s10803-018-3791-7
Sneed, L., & Samelson, D. (2022). Effectiveness of parent-led applied behavior analysis at improving outcomes for parents of autistic children. Journal of Social, Behavioral, and Health Sciences, 16(1), 160-176. https://doi.org/10.5590/JSBHS.2022.16.1.12
Steinbrenner, J. R., Hume, K., Odom, S. L., Morin, K. L., Nowell, S. W., Tomaszewski, B., Szendrey, S., McIntyre, N. S., Yucesoy-Ozkan, S., & Savage, M. N. (2020). Evidence-based practices for children, youth, and young adults with Autism. The University of North Carolina at Chapel Hill, Frank Porter Graham Child Development Institute, National Clearinghouse on Autism Evidence and Practice Review Team. https://ncaep.fpg.unc.edu/sites/ncaep.fpg.unc.edu/files/imce/documents/EBP%20Report%202020.pdf
Tsermentseli, S., & Kouklari, E. C. (2021). Impact of child factors on parenting stress of mothers of children with autism spectrum disorder and intellectual disability: A UK school-based study. Early Child Development and Care, 191(10), 1555-1566. https://doi.org/10.1080/03004430.2019.1658090
Viljoen, M., Mahdi, S., Shelly, J., & de Vries, P. J. (2021). Parental perspectives of functioning in their children with autism spectrum disorder: A global scoping review. Autism: the international journal of research and practice, 25(1), 176-198. https://doi.org/10.1177/1362361320950055
Virués-Ortega J. (2010). Applied behavior analytic intervention for autism in early childhood: meta-analysis, meta-regression and dose-response meta-analysis of multiple outcomes. Clinical Psychology Review, 30(4), 387-399. https://doi.org/10.1016/j.cpr.2010.01.008
Vismara, L. A., McCormick, C. E. B., Wagner, A. L., Monlux, K., Nadhan, A., & Young, G. S. (2018). Telehealth parent training in the Early Start Denver Model: results from a randomized controlled study. Focus on Autism and Other Developmental Disabilities, 33(2), 67-79. https://doi.org/10.1177/1088357616651064
Wilkes-Gillan, S., & Lincoln, M. (2018). Parent-mediated intervention training delivered remotely for children with autism spectrum disorder (ASD) has preliminary evidence for parent intervention fidelity and improving parent knowledge and children's social behaviour and communication skills. Australian Occupational Therapy Journal, 65(3), 245-246. https://doi.org/10.1111/1440-1630.12481
Wong, C., Odom, S. L., Hume, K. A., Cox, A. W., Fettig, A., Kucharczyk, S., Brock, M. E., Plavnick, J. B., Fleury, V. P., & Schultz, T. R. (2014). Evidence-based practices for children, youth, and young adults with autism spectrum disorder. The University of North Carolina, Frank Porter Graham Child Development Institute, Autism Evidence-Based Practice Review Group. https://autismpdc.fpg.unc.edu/sites/autismpdc.fpg.unc.edu/files/imce/documents/2014-EBP-Report.pdf
Wong, C., Odom, S. L., Hume, K. A., Cox, A. W., Fettig, A., Kucharczyk, S., Brock, M. E., Plavnick, J. B., Fleury, V. P., & Schultz, T. R. (2015). Evidence-based practices for children, youth, and young adults with autism spectrum disorder: a comprehensive review. Journal of Autism and Developmental Disorders, 45(7), 1951-1966. https://doi.org/10.1007/s10803-014-2351-z
Disponibilidade de dados: O conjunto de dados que embasa os resultados deste estudo não está disponível.
Como citar: Emilio, A. R., & Portes. J. R. M. (2024). Modelo híbrido de treinamento parental para mães de crianças pré-escolares com transtorno do espectro autista baseado na análise do comportamento aplicada para redução do estresse parental. Ciencias Psicológicas, 18(2), e-3285. https://doi.org/10.22235/cp.v18i2.3285
Contribuição de autores (Taxonomia CRediT): 1. Conceitualização; 2. Curadoria de dados; 3. Análise formal; 4. Aquisição de financiamento; 5. Pesquisa; 6. Metodologia; 7. Administração do projeto; 8. Recursos; 9. Software; 10. Supervisão; 11. Validação; 12. Visualização; 13. Redação: esboço original; 14. Redação: revisão e edição.
A. R. E. contribuiu em 1, 2, 3, 4, 5, 6, 7, 8, 11, 12, 13, 14; J.R.M.P. em 3, 6,7, 8, 10, 12, 14.
Editora científica responsável: Dra. Cecilia Cracco.
10.22235/cp.v18i2.3285
Original Articles
Hybrid model of parent training for mothers of preschool children with autism spectrum disorder based on applied behavior analysis to reduce parental stress
Modelo híbrido de treinamento parental para mães de crianças pré-escolares com transtorno do espectro autista baseado na análise do comportamento aplicada para redução do estresse parental
Modelo híbrido de entrenamiento parental para madres de niños en edad preescolar con trastorno del espectro autista basado en el análisis de comportamiento aplicado para reducir el estrés parental
Aline Regina Emilio1, ORCID 0009-0007-1654-866X
João Rodrigo Maciel Portes2, ORCID 0000-0003-2512-4491
1 Universidade do Vale do Itajaí, Brazil, [email protected]
2 Universidade do Vale do Itajaí, Brazil
Abstract:
This study sought to evaluate the contributions of a hybrid parental training carried out with eight mothers of preschool children with autism spectrum disorder, based on the science of applied behavioral analysis for reducing parental stress. The hybrid parental training was constructed and implemented by the researchers. The sample was divided into two groups: a Treatment Group and a Control Group. In the data analysis, comparisons were made of the levels of stress pre- and post-intervention and for the treatment group, direct practice with the child in a face-to-face environment was also analyzed. The results showed that the mothers in the treatment group reacted positively to the video and materials presented; however, no significant statistical differences were found that would suggest a reduction in stress levels between the two groups as a result of the training given. The limitations of the study were its small sample size and the fact that the children in both groups continued to receive intensive therapy treatment during the application of the parental training.
Keywords: autism; parent training; telehealth; applied behavior analysis; parental stress.
Resumo:
Este estudo buscou avaliar as contribuições de um treinamento parental híbrido realizado com oito mães de crianças pré-escolares com transtorno do espectro do autismo baseado na ciência da análise do comportamento aplicada para a redução do estresse parental. Foi realizado a construção e implementação do treinamento parental híbrido. A amostra foi dividida em grupo tratamento e controle. Em termos de análise de dados, foram feitas comparações do nível de estresse no período pré/pós-intervenção, assim como a análise de uma prática direta com a criança de forma presencial com o grupo tratamento. Os resultados obtidos demonstraram que as mães do grupo tratamento reagiram positivamente com as vídeos e materiais apresentados. No entanto, não foi observado diferenças estatísticas significativas para sugerir a redução do nível de estresse entre os dois grupos. As limitações do estudo foram o tamanho reduzido da amostra e o fato das crianças de ambos os grupos continuarem recebendo o tratamento em terapia intensiva durante a aplicação do treinamento parental.
Palavras-chave: autismo; treinamento de pais; telessaúde; análise do comportamento aplicada; estresse parental.
Resumen:
Este estudio buscó evaluar los aportes de un entrenamiento parental híbrido realizado con ocho madres de niños preescolares con trastorno del espectro autista basado en la ciencia del análisis aplicado de la conducta para la reducción del estrés parental. Se llevó a cabo la construcción e implementación de un entrenamiento parental híbrido. Se dividió la muestra en grupo de tratamiento y control, y se realizaron comparaciones del nivel de estrés en el período pre/postintervención, así como el análisis de la práctica directa con el niño en un cara a cara con el grupo de tratamiento. Los resultados obtenidos demuestran que las madres del grupo de tratamiento reaccionaron positivamente a los videos y materiales presentados; sin embargo, no se observaron diferencias estadísticas significativas que sugieran una reducción en el nivel de estrés entre los dos grupos. Las limitaciones del estudio fueron el pequeño tamaño de la muestra y el hecho de que los niños de ambos grupos continuaron recibiendo tratamiento de terapia intensiva durante la implementación de la capacitación de los padres.
Palabras clave: autismo; formación de padres; telesalud; análisis aplicado del comportamiento; estrés parental.
Received: 10/03/2023
Accepted: 21/06/2024
According to the Diagnostic and Statistical Manual of Mental Disorders (5th ed.) (DSM-5 TR; American Psychiatric Association, 2023) autism spectrum disorder (ASD) is a neurodevelopment disorder characterized by persistent deficits in social interaction, repetitive behavioral patterns and restricted interests, and these symptoms must be present in early childhood, with different levels of support. The prevalence of ASD has been increasing exponentially. According to an epidemiological study carried out by the Centers for Disease Control and Prevention (2023), one in every thirty-six children in the USA currently has ASD.
The difficulties presented by children diagnosed with ASD not only impact the individual, but also those who live with them, especially their parents or caregivers (Dahiya et al., 2021). Parents of children with ASD suffer from high levels of parental stress when compared to parents of children with other disabilities or those with typical development (Craig et al., 2016). Children with ASD demand more time and care from their parents and caregivers. This can have a direct effect on the lives of all those involved, especially the mothers, on whom the burden is greatest, and who often give up their own personal interests and social lives to devote themselves to the care of their children (Anjos & Morais, 2021; Portes & Vieira, 2022).
One strategy to help parents face the challenges involved in caring for children with ASD is parental training, which offers a promising alternative that is feasible, well-accepted, and relatively low in cost (Dawson-Squibb et al., 2020). Parental training can also help reduce the emotional burden and parental stress (Kurzrok et al., 2021; Sneed & Samelson, 2022). Parental stress levels in parents of children with ASD are generally related to the child's behavior, barriers to participation in social and educational activities, or concerns about treatments (Shepherd et al., 2018).
Parental training can be defined as a strategy that aims to teach parents how to identify disruptive behaviors, analyze the function of these behaviors, adopt preventative strategies, manage such behaviors, and learn how to communicate better with the child. The training techniques include video modeling, roleplay, and direct instructions through expository classes and complementary materials (Wong et al., 2014).
Applied Behavioral Analysis (ABA) is currently indicated as one of the main sciences that has made a significant contribution to early intervention in ASD (Sella & Ribeiro, 2018). The interventions under this theoretical framework constitute an evidence-based practice for this population (Steinbrenner et al., 2020; Virués-Ortega, 2010; Wong et al., 2015). Although there is vast literature that presents evidence of the effectiveness of parental training in families with children diagnosed with ASD from an ABA perspective (Lee & Meadan, 2020; Lopes et al., 2021; Nevill et al., 2018; Rahman et al., 2016; Wong et al., 2015), the impacts of this training on mental health indicators are moderate, and more scientific production is needed on the subject (Mackenzie & Eack, 2022).
Families of children with ASD in locations with low resources encounter various barriers, such as the poor qualification of professionals in this field, a lack of public health infrastructure, the high cost of mental health services, social representations about the disorder, and greater geographical distance from the nearest specialized centers (Dawson- Squibb et al., 2020; Viljoen et al., 2021). Therefore, implementing parental training for parents of children with ASD using information and communication technologies (ICTs), through the use of telepractice offers a low-cost means of enabling access to evidence-based treatments and developing social and communication skills of children with ASD (Camden et al., 2019; Parsons et al., 2017; Wilkes-Gillan & Lincoln, 2018). Despite the lack of technological applications for children with disabilities, the available studies report promising results for children with ASD (Samadi et al., 2020; Vismara et al., 2018).
Telepractice is a general term that embraces other terms, such as telehealth and telemedicine. It can be defined as a means of providing distance professional services through the use of the internet (Meadan et al., 2022). Telepractice can be offered in two forms: asynchronous and synchronous. The first is when information, such as videos, photos, or audio files are recorded and exchanged via technology between the therapist and the client without any live interaction between them, and the second is when there is real-time interaction through ICTs. When synchronous and asynchronous methods are used in combination, this is called hybrid telepractice, which combines the benefits of both synchronous and asynchronous approaches (Dudding, 2013). The combination of telepractice strategies with face-to-face teaching – the form adopted in this research – is also considered a hybrid model.
Based on this panorama, this study aimed to evaluate the contributions of a hybrid model of parental training for mothers of preschool children with ASD, based on ABA, aimed at reducing parental stress.
Method
This study is characterized as a non-randomized (quasi-experimental) clinical trial. It is part of a master’s degree dissertation reporting on research approved the Ethics Committee of the University of Vale do Itajaí on 25/04/2022, under no. 5,366,120. In this type of clinical trial, the exposure of independent variables to the participants is controlled, and there is no randomization between the groups (Hernandez-Sampieri et al., 2013).
Participants
The study sample was formed by convenience. Eight mothers participated in the study, ranging from 34 to 44 years of age. Their children, all diagnosed with ASD, had a mean age of 3.75. The children had been undergoing behavioral intervention at a specialized center in the South of Brazil for approximately eight months. More information about the sample is shown in Table 1 (sample characterization) and Table 2 (data on the children of the sample).
Instruments
Socio-demographic questionnaire: an instrument constructed by the researchers, with the aim of eliciting information about the children and mothers participating in the research. The questionnaire sought to characterize the children according to: sex, age, year of diagnosis, school situation, total length of time the child had been in intervention, and length of time at the center. The mothers were characterized by place of birth, marital status, level of education, profession, family income, number of children, members of the household, and caregivers of the child, and whether they were receiving psychological follow-up.
Videoconference Checklist: A document created by researchers to be used as a script during the videoconferences held with mothers of the treatment group, in order to standardize the online meetings. This included reminders, such as keeping the videoconference to a maximum of ten minutes, guidelines on how to conduct the meeting, and the information that should be collected.
In-person practical training script: this was created entirely by the researchers so that during the in-person meetings, the researchers could observe the participants’ skills in implementing the practices taught in the videos. The document presented a series of requests for the researcher to ask the participant. If the request was carried out by the participant, the researcher moved on to the next. Or if the participant had difficulty performing the request, the researcher gave assistance. The requests provided opportunities to consolidate the contents shown in the videos, with the participants putting them into actual practice with their children. Skills were reinforced such as engaging the child, motivation, reinforcement, instruction, token economy, types and help, incidental and subtle forms of teaching, behavior function, managing inappropriate behavior, and imitation. The script also gave information on what the researcher should do if the child presented inappropriate behavior.
Protocol for observing in-person training: This protocol was created entirely by the authors, with closed questions on a Likert scale through which the observers were able to analyze the mothers’ performance during the videos of the in-person training. This document was related to the Roadmap of practical in-person training, as it enabled the researchers to evaluate whether participants were able to perform the tasks they were asked to carry out, and whether they did so independently, or needed some kind of help from the researcher (modeling or verbal).
Social Responsiveness Scale (SRS-2): This is a
Likert scale composed of different forms for different age groups. It seeks to
quantitatively and reliably quantify a wide range of possible losses of
socialization, communication, repetitive behaviors and restricted interests
that may be associated with ASD, and present the level of symptoms: mild,
moderate or severe, through the responses filled out by the parents or teachers.
The SRS-2 is composed of sixty-five measurements (Constantino & Gruber,
2020). The validation studies for the Brazilian context of this scale
demonstrate psychometric properties with values of consistency ![]() = .95 and
= .95 and ![]() = .97, sensitivity of 96.8 %, specificity of 100 %
and a negative predictive value of 99.99 % for the identification of ASD
(Borges & Hauck-Filho,).
= .97, sensitivity of 96.8 %, specificity of 100 %
and a negative predictive value of 99.99 % for the identification of ASD
(Borges & Hauck-Filho,).
Parental Stress Index – Short Form: To evaluate parental stress, the Portuguese adaptation of the Parental Stress Index – Short Form (PSI-SF) was used. It consists of thirty-six items, and is divided into three subcategories: difficult child; parental suffering; and dysfunctional interactions (Santos, 2008). The validation study of PSI-SF in Portugal (Santos, 2008) presents psychometric properties, with Cronbach's alpha coefficient of .92. The instrument has not yet been validated for Brazil context, but since Brazil and Portugal share the same language, it was decided to use this scale, due to a lack of evaluation instruments in this area validated for Brazil.
Procedures
Hybrid Parental Training
The proposal for training parents of children with ASD was constructed according to the following steps: A) discussion among researchers on parental training in hybrid format for parents/caregivers of preschool children diagnosed with ASD, b) a review of the literature on the subject over the last five years, c) deciding on the contents of each video, d) preparing the visual material (slides) to be presented in the videos, recording and editing the videos, e) checking and correcting the videos, f) making the videos available, g) applying the parental training, and h) evaluating their effectiveness.
The topics covered in the training were: 1) What is Autism Spectrum Disorder and the ABA used with this demand, 2) basic principles such as reinforcement, punishment, and extinction, among others, 3) What is behavior, how to define it, and its possible functions, 4) How to establish motivating operation and carry out a preference assessment with the child, 5) systems to assist in the teaching of skills (system of tips) and how to present instructions clearly and if necessary, redirect behavior, 6) differential reinforcement strategies applied in daily life, 7) the importance of play and the possibilities of playing and teaching with the child, 8) how to set up and perform a schedule of activities with the child, and the importance of and how to establish instructional control, 9) the difference between naturalistic and structured teaching, and how to apply each.
Examples and practical relationship with daily life were presented in the videos, in clear language, explaining any technical terms with terms that could be more easily understood by the mothers. Each video lasted approximately forty minutes. Themes 1-6 were contained in two videos, and the others, in one video. All the videos were made available on YouTube, via a private link. Throughout the training, the mothers of the treatment group continued to have access to the videos they had already watched.
Data collection
First step
Initially the researcher sent an invitation via WhatsApp to the parents or guardians of children who attended the center, inviting them to take part in the research. The mothers who accepted the invitation (by replying to the message) and who met the study inclusion criteria, took part. The inclusion criteria were: a child diagnosed with ASD, from mild to severe, according to the Social Responsiveness Scale (SRS-2); a child who had been in early intervention at the center for the past 6 to 12 months; child aged between 2 years 6 months and 6 years; participants who had not previously received training or courses in applied behavior analysis; access to the Internet; literate; had time to attend the center. The exclusion criteria were: a neurodevelopmental deficiency or disorder that could prevent the individual from attending and participating in the training classes or responding to the instruments.
The groups were divided randomly. The first four mothers who agreed to participate in the research were assigned to the Treatment Group, and the remainder to the Control Group. A visit was scheduled with each participant, to come to the center, where they were asked to sign an Informed Consent Form – ICF. The sociodemographic questionnaire, SRS-2, and the Parental Stress Index (PSI) were also applied. In this visit, only the mothers of the Treatment Group received instructions from the researcher on the process of the program, and how to access the videos (approximately 30/40 minutes each), on different themes related to ASD and ABA.
The mothers were asked to watch two videos of two modules per week in the next seven days. After they had watched the videos, a video conference with the researcher was scheduled and conducted. After that, two more modules were made available. However, some mothers were unable to watch all the videos within the established deadline, so a period of fifteen days was given, for the mothers to watch the videos and attend the videoconference. This procedure continued, until a final face-to-face meeting was carried out. This meeting included the practical part, which was recorded for analysis by the researcher. The entire process took 13 weeks.
For the four participants of the Control Group, the researcher listened to any requests the participants had, and they were informed that they would receive messages via WhatsApp, to monitor the case, and that any requests would be forwarded to the technical team responsible for the child's care at the center. The mothers were also informed that they would receive the same training once the research was completed.
Second step
After the first stage, the mothers watched the first two videos and took part in the videoconference. During the videoconference with the participants of the Treatment Group, a videoconference checklist was administered and the subsequent videos were made available for them to watch. This procedure was repeated fortnightly, until the participants had finished watching all the videos. Next, an in-person meeting was scheduled, to carry out the practical part of the training.
Third step
In the third stage of data collection, the researcher and the participants of the Treatment Group attended the center individually, with their children, where the practical part of the training was carried out. This session was recorded for observation by the judges.
The meeting took place in a room equipped with two cameras to capture audio and video. The sessions lasted no more than twenty minutes, and followed the itinerary for the hands-on training. At the end of the session, the participant was referred to another room in which the Parental Stress Index-Short Form (PSI-SF) was applied again.
Fourth step
Two judges with training and experience in ABA, employees of the intervention center where the research took place, performed an independent analysis of the four recorded videos of the practical face-to-face sessions with the participants of the Treatment Group. For the analysis they followed the protocol of observation of the practical training in face-to-face.
Data analysis
First, the information collected through the sociodemographic questionnaire was organized, tabulated and analyzed descriptively, in order to characterize the participants’ profile in relation to the research objectives.
The data obtained from the Parental Stress Index-Short Form (PSI-SF) were analyzed using descriptive statistics, seeking to describe a set of data, and through inferential statistics, aiming to understand, compare and draw conclusions on the responses to the questionnaires applied to the research participants (Dancey & Reidy, 2019). The Wilcoxon non-parametric tests were used to evaluate intragroup differences and the Mann Whitney test was used to analyze the differences between the Treatment and Control Groups (Dancey & Reidy, 2019).
The video recordings of the in-person training with the participants were analyzed individually, through the observation protocol of the hands-on training, counting the occurrence of each item of this instrument during the training. The first three minutes of the videos were disregarded from the analysis, as this period was allowed for the mothers and children to settle themselves in the care room. The rest of the video time was coded.
To verify the reliability of the instrument for observing the participants’ behavior during the training, the analyses of two expert judges were used, each with more than 2 years of experience in ABA. They were instructed on the use of the protocol for observation of the practical in-person training. They watched the videos independently, and through the protocol, identified whether or not the participants presented behaviors requested by the researcher. In the items where they did not correctly present these behaviors, the researcher acted as a third judge, and analyzed the items to make the final decision.
In general, inter-observer agreement should be at least 80 %. To obtain the level of agreement, the following formula was applied: ∑A/ ∑(A+D) x 100 after each judge had analyzed each video. An overall average of 95.45 % was obtained for inter-observer agreement.
Results and Discussion
Analyzing the demographic data of the participants (Table 1), it was found that all were in a marital relationship with the child's father, and living together with their spouse. The analysis also found a high level of education, with seven of the mothers having degrees or postgraduate degrees. Only the participant P-3 had completed high school but not higher education. Regarding family income, it was above R$4001 per month, with some participants having income of more than R$7000 per month. These data imply that the mothers had good access to information about autism and quality intervention, which suggests lower levels of parental stress, as cross-sectional factors beyond ASD, such as conflicts in the marital relationship, lack of support network, lack of public policies to ensure care for children with ASD, low socioeconomic level and low levels of education are all negative factors for the mental health of family members (Anjos & Morais, 2021).
Also in regard to the participants’ information, it was observed participant P-1 was not in employment at the time of the research.
The results of the SRS-2 scale (Table 2), which evaluated the level of support of children through the mothers’ responses, showed that 3 of the 8 children receive mild support level, and the others moderate support. Through the existing literature, it is possible to verify that the higher the level of support the child needs, the higher the manifestation of symptoms, which could be related to parental stress (Hartley et al., 2017).
It was observed that participant P-5 of the Control Group presented the lowest stress scores on the scale (pre-test score 67/post-test score 73). However, this was also the only case in which the participant of the research was not the main caregiver of the child. He was a father (who did not participate in the research), and another fact is that the mother had worked full-time since the child was diagnosed, while the father had stayed at home to look after the child. Usually, the father is not the primary caregiver of the child with ASD, and does not carry out basic care activities (Jorge et al., 2021).
Table 1: Characterization of the sample (N = 8)
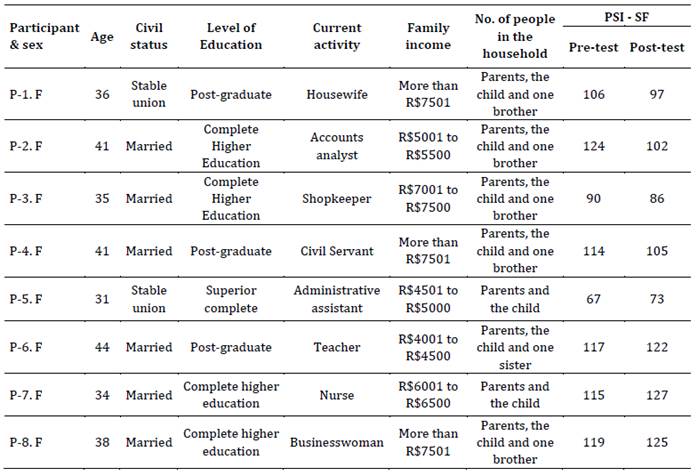
Table 2: Characterization of the children of the sample (N = 8)
Note: F: Female; M: Male
The results obtained from the PSI-SF scale were tabulated in an Excel spreadsheet, and calculations were performed to obtain the mean and standard deviations for each individual and group, both pre- and post-intervention. Wilcoxon's non-parametric tests were used to compare the groups in both stages of the research (pre- and post-intervention). These data are presented in Table 3. The Mann-Whitney test was used to compare the results between groups.
Table 3: PSI-SF pre/post-test result
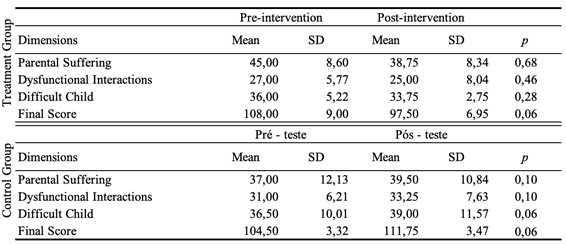
The research involved 8 participants, all female, with a mean age of 37.5 years, all mothers of children diagnosed with ASD at preschool age. It was assumed that the mother is the primary caregiver of the child (Machado et al., 2018), which is what we found in this research. As the main caregivers, it is common for mothers to suffer from excessive burden, lack of support, health issues, and impact on their lives and relationships. These aspects were evaluated through the Parental Suffering dimension of the PSI-SF.
In this dimension, initially the scores of the participants of the same group were compared for both stages (pre/post) and both groups did not present any statistically significant differences (p < 0), and in the comparisons of the means between groups for this same dimension, in the pre-intervention the mean for the treatment group, of M = 45.00 (SD = 8.60), was greater than the mean of the control group M = 37.00 (SD = 12.130, the post-intervention mean for the treatment group was M = 38.75 (SD = 8.34), thus, the mean decreased so that it was less than that of the control group, which was M = 39.50, thus, it increased in the post-intervention. Despite this, there was no statistically significant difference between the two groups (U = 0.48; p < 0).
Collaborating with Parental Suffering, some studies suggest that mothers of children with ASD suffer greater impacts on their lives, including on their physical, mental and/or professional health, due to the intensive care needs of the child, leading to feelings of being overburdened (Machado et al. 2018).
In the dimension of dysfunctional interactions, the parents' expectations of the relationship with the child are evaluated; the possibility of being reinforced, accepted, bonding with their child, that is, and the level of relational satisfaction with the child. Comparing the results of the participants in the same group, there were no significant differences (p < 0), and the same occurred when comparing between groups (U = 1; p < 0). This result reveals that the mothers’ sense of being unable to build a close relationship with their children diagnosed with ASD, which may threaten the mother's own sense of identity and contribute to maternal stress (Porter & Loveland, 2019). Increasing the interaction between parents and children, as well as the feeling of being connected, can contribute to reducing the level of stress (Anjos & Moraes, 2021).
The last dimension is called Difficult Child, and its affirmations are related to the characteristics of the child, such as humor, hyperactivity, requirement, adaptability, acceptance, autonomy, and how much these characteristics impact the parents’ lives. In the intra-group comparison, no results were obtained with statistical significance (p < 0), or when comparing the results for both groups (U = 1; p < 0), as in the post-test (U = 0,68), suggesting that the mothers’ perception of their children and their children’s behaviors is similar for both groups. These results reinforce the link between the mothers’ stress levels and the severity of the central symptoms of their children with ASD. The literature also indicates a close relationship between parental stress and the characteristics/symptomatology of ASD (Siu et al., 2019; Tsermentseli & Kouklari, 2021).
In the sum of the dimensions (final score), and in the analysis among the participants of the treatment group, no statistical relevance was found (p < 0). Comparing the means of the final scores in both stages, in the pre-test the treatment group presented M = 108,00 (SD = 9.00), which is higher than that of the control group M = 104.50 (SD = 3.32). However, in the post-test performed shortly after the parental training, the treatment reduced the mean score to M = 97.50 (SD = 6.95), while the treatment group increased the mean score to M = 111.75 (SD = 3.47). And between groups (U = 0.68; p < 0) and the post-intervention (U = 0.34; p < 0) which did not suggest significance, therefore it was concluded that there were no differences that could suggest that the treatment group’s participation in the hybrid parental training had a significant impact on the level of stress, when comparing through statistical analysis.
This research, as well as others on parental training, did not find any evidence to support a significant change in parental stress in the study population (DAI et al., 2018; Fisher et al., 2020; Mackenzie & Eack, 2022). This may be associated with the fact that the children were in intervention and the participants were assisted by professionals specialized in ASD, or that stress is influenced by different variables, such as the characteristics of the individual caregiver, the characteristics of the child, the family structure and dynamic, bonds established between the caregiver and the child, social and socioeconomic factors, support network, ability to access quality information and intervention, cultural context, among others (Louie et al., 2017). To affirm that parental training can help reduce stress levels, these variables would need to be studied in greater depth.
It is important to emphasize the importance of instrumentalizing and empowering parents and caregivers of children with ASD. Despite the absence of statistical evidence of its effectiveness, the individuals of the treatment group gave positive opinions, such as that the techniques taught can be introduced into their routines, that the content was interesting and necessary, and that it would help them in different aspects, such as managing disruptive behaviors, generalization and teaching new skills. This contributes directly to the development of the child and improves the family context, and by broadening the understanding of the whole process involving ASD, it can make a significant contribution not only to lowering the levels of parental stress, but also levels of anxiety and depression, giving the mothers hope (Liu et al. 2021).
Final considerations
The main objective of this research was to evaluate the contributions of a hybrid model of parental training for mothers of preschool children with ASD based on ABA for parental stress reduction. It is concluded, after listening to the participants of the treatment group, that the training made an important contribution to their routines. It was also observed that in the practical session with the researcher, the participants were able to implement the techniques properly. These were qualitative results of the research, although it is not possible to affirm that the group that received training had a reduction in parental stress compared to the control group.
A parental training model under the principles of ABA can help raise awareness among parents of the ways in which they can assist the development of their children, give them effective ways to teach new skills or manage disruptive behavior, increase parents’ knowledge, and minimize the impact of parental stress. It is recommended that this training be applied to other caregivers, to evaluate its effects on lowering parental stress. Parental training is a low-cost tool, and when carried out in the hybrid format, it becomes more accessible to families.
This study also presents some limitations; one is the small sample (N = 8), which significantly compromised the validity of the findings; another is that the mothers accompany their children in a specialized and private institution. Other variables that may have contributed to the comparison of pre/post-intervention stress were not investigated thoroughly, for example marital relationship, mother’s mental health, the demands of having to care for other children, and the caregiver’s perception of the child with ASD, among others. Another limitation we encountered was that the researcher had already had previous opportunities to work with the children who composed the sample, and present instructional control with them, and this may have prompted the children to present the expected behavior during the practical in-person training. Also, the fact that children were already receiving intensive and regular interventions, at the center, based on ABA, was an intervening variable.
Given the above, it is suggested this research be replicated, taking into account the necessary changes related to the limitations presented, in order to obtain better results.
References:
American Psychiatric Association. (2023). DSM-5TR: Manual diagnóstico e estatístico de transtornos mentais (5ª ed. Revisado). Artmed.
Anjos, B. B., & Morais, N. A. (2021). As experiências de famílias com filhos autistas: uma revisão integrativa da literatura. Ciências Psicológicas, 15(1), e2347. https://doi.org/10.22235/cp.v15i1.2347
Borges, L. & Hauck-Filho, N. (2020). Escala de Responsividade Social (SRS-2). Hogrefe.
Camden, C., Pratte, G., Fallon, F., Couture, M., Berbari, J., & Tousignant, M. (2020). Diversity of practices in telerehabilitation for children with disabilities and effective intervention characteristics: results from a systematic review. Disability and rehabilitation, 42(24), 3424-3436. https://doi.org/10.1080/09638288.2019.1595750
Centers for Disease Control and Prevention. (2023). CDC Launches Autism Data Visualization Tool to Improve Access to Data. https://www.cdc.gov/ncbddd/autism/index.html
Constantino, J. N., & Gruber C. P. (2020). SRS II: Escala de Responsividade Social. Hogrefe.
Craig, F., Operto, F. F., De Giacomo, A., Margari, L., Frolli, A., Conson, M., Ivagnes, S., Monaco, M., & Margari, F. (2016). Parenting stress among parents of children with Neurodevelopmental Disorders. Psychiatry Research, 242, 121-129. https://doi.org/10.1016/j.psychres.2016.05.016
Dahiya, A. V., Openden, D., Ostmeyer, K. F., Anderson, R. M., & Scarpa, A. (2021). Pivotal response treatment for autism: A brief report on training for rural communities. Journal of Community Psychology, 49(7), 2983-2994. https://doi.org/10.1002/jcop.22558
Dai, Y. G., Brennan, L., Como, A., Hughes-Lika, J., Dumont-Mathieu, T., Rathwell, I. C., Minxhozi, O., Aliaj, B., & Fein, D. A. (2018). A video parent-training program for families of children with autism spectrum disorder in Albania. Research in autism spectrum disorders, 56, 36-49. https://doi.org/10.1016/j.rasd.2018.08.008
Dancey, C., & Reidy, J. (2018). Estatística Sem Matemática para Psicologia. Penso.
Dawson-Squibb, J. J., Davids, E. L., Harrison, A. J., Molony, M. A., & de Vries, P. J. (2020). Parent education and training for autism spectrum disorders: Scoping the evidence. Autism: the international journal of research and practice, 24(1), 7-25. https://doi.org/10.1177/1362361319841739
Dudding, C. (2013). Reimbursement and telepractice. Perspectives on Telepractice, 3, 35-40. https://doi.org/10.1044/teles3.2.35
Fisher, W. W., Luczynski, K. C., Blowers, A. P., Vosters, M. E., Pisman, M. D., Craig, A. R., Hood, S. A., Machado, M. A., Lesser, A. D., & Piazza, C. C. (2020). A randomized clinical trial of a virtual-training program for teaching applied-behavior-analysis skills to parents of children with autism spectrum disorder. Journal of Applied Behavior Analysis, 53(4), 1856-1875. https://doi.org/10.1002/jaba.778
Hartley, S. L., Papp, L. M., Mihaila, I., Bussanich, P. M., Goetz, G., & Hickey, E. J. (2017). Couple conflict in parents of children with versus without Autism: self- reported and observed findings. Journal of Child and Family Studies, 26(8), 2152-2165. https://doi.org/10.1007/s10826-017-0737-1
Hernández-Sampieri, R., Fernández-Collado, C., & Baptista Lucio, P. (2013). Metodologia da Pesquisa (5a ed.). Penso.
Jorge, G. H., Santos, Y. L. C. M., Portes, J. R. M., & Bossardi, C. N. (2021). Envolvimento paterno de pais de crianças com o Transtorno do Espectro Autista. Boletim - Academia Paulista de Psicologia, 41(101), 175-184. https://doi.org/10.5935/2176-3038.20210018
Kurzrok, J., McBride, E., & Grossman, R. B. (2021). Autism-specific parenting self-efficacy: An examination of the role of parent-reported intervention involvement, satisfaction with intervention-related training, and caregiver burden. Autism: the international journal of research and practice, 25(5), 1395-1408. https://doi.org/10.1177/1362361321990931
Lee, J. D., & Meadan, H. (2020). Parent-mediated interventions for children with ASD in low-resource settings: a scoping review. Review Journal of Autism and Developmental Disorders, 8(3), 285-298. https://doi.org/10.1007/s40489-020-00218-7
Liu, G., Wang, S., Liao, J., Ou, P., Huang, L., Xie, N., He, Y., Lin, J., He, H. G., & Hu, R. (2021). The efficacy of WeChat-Based Parenting Training on the psychological well-being of mothers with children with autism during the COVID-19 pandemic: quasi-experimental study. JMIR Mental Health, 8(2), e23917. https://doi.org/10.2196/23917
Lopes, V. D., Murari, S. C., & Kienen, N. (2021). Capacitação de pais de crianças com TEA: revisão sistemática sob o referencial da Análise do Comportamento. Revista Educação Especial, 34, e19, 1-28. https://doi.org/10.5902/1984686X43768
Louie, A. D., Cromer, L. D., & Berry, J. O. (2017). Assessing parenting stress: Review of the use and interpretation of the Parental Stress Scale. The Family Journal, 25(4), 359-367. https://doi.org/10.1177/1066480717731347
Machado, M. S., Londero, A. D., & Pereira, C. R. R. (2018). Tornar-se família de uma criança com transtorno do espectro autista. Contextos Clínicos, 11(3), 335-350. https://dx.doi.org/10.4013/ctc.2018.113.05
Mackenzie, K. T., & Eack, S. M. (2022). Interventions to improve outcomes for parents of children with autism spectrum disorder: a meta-analysis. Journal of Autism and Developmental Disorders, 52, 2859-2883. https://doi.org/10.1007/s10803-021-05164-9
Meadan, H., Lee, J. D., & Chung, M. Y. (2022). Parent-implemented interventions via telepractice in autism research: A review of social validity assessments. Current Developmental Disorders Reports, 9(4), 213-219. https://10.1007/s40474-022-00259-z
Nevill, R. E., Lecavalier, L., & Stratis, E. A. (2018). Meta-analysis of parent-mediated interventions for young children with autism spectrum disorder. Autism: the international journal of research and practice, 22(2), 84-98. https://doi.org/10.1177/1362361316677838
Parsons, D., Cordier, R., Vaz, S., & Lee, H. (2017). Parent-mediated intervention training delivered remotely for children with autism spectrum disorder living outside of urban areas: systematic review. Journal of Medical Internet Research, 19(8), e198. https://doi.org/10.2196/jmir.6651
Porter, N., & Loveland, K. A. (2019). An integrative review of parenting stress in mothers of children with autism in Japan. International Journal of Disability, Development and Education, 66(3), 249-272. https://doi.org/10.1080/1034912X.2018.1439159
Portes, J. R. M., & Vieira, M. L. (2022). Percepção parental sobre o filho com autismo: as repercussões na adaptação familiar. Revista Psicologia em Pesquisa, 16(2), 1-23. http://dx.doi.org/10.34019/1982-1247.2022.v16.32614
Rahman, A., Divan, G., Hamdani, S. U., Vajaratkar, V., Taylor, C., Leadbitter, K., Aldred, C., Minhas, A., Cardozo, P., Emsley, R., Patel, V., & Green, J. (2016). Effectiveness of the parent-mediated intervention for children with autism spectrum disorder in south Asia in India and Pakistan (PASS): a randomised controlled trial. The Lancet. Psychiatry, 3(2), 128-136. https://doi.org/10.1016/S2215-0366(15)00388-0
Samadi, S. A., Bakhshalizadeh-Moradi, S., Khandani, F., Foladgar, M., Poursaid-Mohammad, M., & McConkey, R. (2020). Using hybrid telepractice for supporting parents of children with ASD during the COVID-19 lockdown: A feasibility study in Iran. Brain Sciences, 10(11), 892. https://doi.org/10.3390/brainsci10110892
Santos, S. V. (2008). Forma reduzada do parenting stress index (PSI): Estudo Preliminar. XII Conferência Internacional Avaliação, Formas e Contextos.
Sella, A. C., & Ribeiro, D. M. (2018). Análise do comportamento aplicada ao transtorno do espectro autista. Appros Editora e Livraria Eireli-ME.
Shepherd, D., Landon, J., Taylor, S., & Goedeke, S. (2018). Coping and care-related stress in parents of a child with autism spectrum disorder. Anxiety, Stress, and Coping, 31(3), 277-290. https://doi.org/10.1080/10615806.2018.1442614
Siu, Q. K., Yi, H., Chan, R. C., Chio, F. H., Chan, D. F., & Mak, W. W. (2019). The role of child problem behaviors in autism spectrum symptoms and parenting stress: A primary school-based study. Journal of Autism and Developmental Disorders, 49, 857-870. https://doi.org/10.1007/s10803-018-3791-7
Sneed, L., & Samelson, D. (2022). Effectiveness of parent-led applied behavior analysis at improving outcomes for parents of autistic children. Journal of Social, Behavioral, and Health Sciences, 16(1), 160-176. https://doi.org/10.5590/JSBHS.2022.16.1.12
Steinbrenner, J. R., Hume, K., Odom, S. L., Morin, K. L., Nowell, S. W., Tomaszewski, B., Szendrey, S., McIntyre, N. S., Yucesoy-Ozkan, S., & Savage, M. N. (2020). Evidence-based practices for children, youth, and young adults with Autism. The University of North Carolina at Chapel Hill, Frank Porter Graham Child Development Institute, National Clearinghouse on Autism Evidence and Practice Review Team. https://ncaep.fpg.unc.edu/sites/ncaep.fpg.unc.edu/files/imce/documents/EBP%20Report%202020.pdf
Tsermentseli, S., & Kouklari, E. C. (2021). Impact of child factors on parenting stress of mothers of children with autism spectrum disorder and intellectual disability: A UK school-based study. Early Child Development and Care, 191(10), 1555-1566. https://doi.org/10.1080/03004430.2019.1658090
Viljoen, M., Mahdi, S., Shelly, J., & de Vries, P. J. (2021). Parental perspectives of functioning in their children with autism spectrum disorder: A global scoping review. Autism: the international journal of research and practice, 25(1), 176-198. https://doi.org/10.1177/1362361320950055
Virués-Ortega J. (2010). Applied behavior analytic intervention for autism in early childhood: meta-analysis, meta-regression and dose-response meta-analysis of multiple outcomes. Clinical Psychology Review, 30(4), 387-399. https://doi.org/10.1016/j.cpr.2010.01.008
Vismara, L. A., McCormick, C. E. B., Wagner, A. L., Monlux, K., Nadhan, A., & Young, G. S. (2018). Telehealth parent training in the Early Start Denver Model: results from a randomized controlled study. Focus on Autism and Other Developmental Disabilities, 33(2), 67-79. https://doi.org/10.1177/1088357616651064
Wilkes-Gillan, S., & Lincoln, M. (2018). Parent-mediated intervention training delivered remotely for children with autism spectrum disorder (ASD) has preliminary evidence for parent intervention fidelity and improving parent knowledge and children's social behaviour and communication skills. Australian Occupational Therapy Journal, 65(3), 245-246. https://doi.org/10.1111/1440-1630.12481
Wong, C., Odom, S. L., Hume, K. A., Cox, A. W., Fettig, A., Kucharczyk, S., Brock, M. E., Plavnick, J. B., Fleury, V. P., & Schultz, T. R. (2014). Evidence-based practices for children, youth, and young adults with autism spectrum disorder. The University of North Carolina, Frank Porter Graham Child Development Institute, Autism Evidence-Based Practice Review Group. https://autismpdc.fpg.unc.edu/sites/autismpdc.fpg.unc.edu/files/imce/documents/2014-EBP-Report.pdf
Wong, C., Odom, S. L., Hume, K. A., Cox, A. W., Fettig, A., Kucharczyk, S., Brock, M. E., Plavnick, J. B., Fleury, V. P., & Schultz, T. R. (2015). Evidence-based practices for children, youth, and young adults with autism spectrum disorder: a comprehensive review. Journal of Autism and Developmental Disorders, 45(7), 1951-1966. https://doi.org/10.1007/s10803-014-2351-z
Data availability: The dataset supporting the results of this study is not available.
How to cite: Emilio, A. R., & Portes. J. R. M. (2024). Hybrid model of parent training for mothers of preschool children with autism spectrum disorder based on applied behavior analysis to reduce parental stress. Ciencias Psicológicas, 18(2), e-3285. https://doi.org/10.22235/cp.v18i2.3285
Authors’ contribution (CRediT Taxonomy): 1. Conceptualization; 2. Data curation; 3. Formal Analysis; 4. Funding acquisition; 5. Investigation; 6. Methodology; 7. Project administration; 8. Resources; 9. Software; 10. Supervision; 11. Validation; 12. Visualization; 13. Writing: original draft; 14. Writing: review & editing.
A. R. E. has contributed in 1, 2, 3, 4, 5, 6, 7, 8, 11, 12, 13, 14; J.R.M.P. in 3, 6,7, 8, 10, 12, 14.
Scientific editor in-charge: Dra. Cecilia Cracco.